Chapter 47 Fat grafting in body contouring surgery
• The most important step in fat grafting the body is analysis of the defect. The bird’s-eye view is an important vantage point.
• Avoiding donor site contour irregularities is best accomplished by limiting the amount of fat harvested from any one area.
• In the body, a 14- to 16-gauge 15 cm Coleman cannula may be used for more efficiency.
• Any existing adhesion that causes surface dimpling needs to be released at the time of fat grafting. It is usually best to release after most of the fat grafting has been performed in order to avoid fat migration.
• Subcutaneous adhesions or scars should be released prior to fat grafting with a V-dissector or W-dissector.
• Fat grafts may increase or decrease in volume over time and it is important that patients understand this preoperatively
Introduction
Structural fat grafting is an essential tool for practitioners performing body contouring surgery. It can be an adjunctive therapy in primary body contouring as well as a corrective modality in iatrogenic corporeal deformities.1–4 A detailed three-dimensional analysis of the areas to be treated is key to successful outcomes.
Surgical Technique
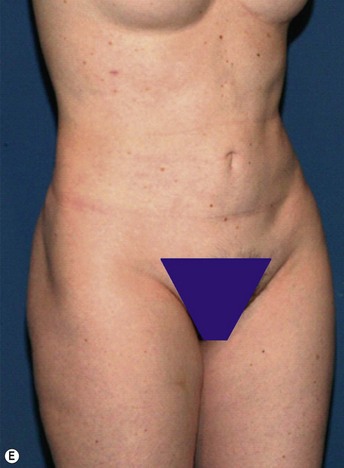
No-one has clearly shown a correlation between donor site location and viability of fat grafts.5,6 For this reason, donor sites are usually selected based on areas whose contour will improve with liposuction. The abdomen and medial thighs are the two most common donor areas.
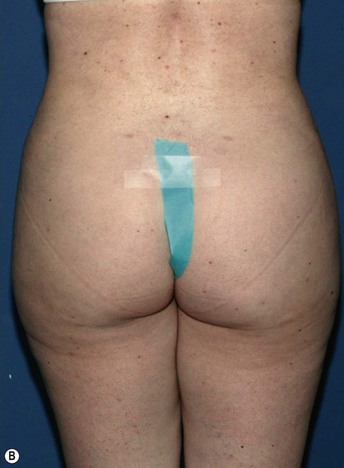
Example: Correction of Buttocks Crease Deformity
Fat placement should obviously be concentrated in the areas of greatest deficiency. However, it is equally important to feather out into surrounding areas to create an integrated correction. In this situation, placement of fat should extend from deep against the muscular fascia to an immediately subdermal plane.7 It is important to avoid linear placement in more superficial planes, as this can cause noticeable lumps.
All areas of infiltration should be approached from at least two directions. This provides more structural integrity as the fat is laid down in a cross-hatched fashion. In this specific situation, access incisions in the buttock and thigh were chosen to allow placement perpendicular and longitudinal to the buttocks crease (Figs 47.1–47.4).
< div class='tao-gold-member'>




Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


