Eyelid Reconstruction With the Hughes Flap or Cutler-Beard Flap
Larissa Habib
Brian P. Marr
DEFINITION
The Hughes flap was originally described in 1937 and has been modified to increase efficacy and minimize postoperative complications.
It is an effective vertical lid-sharing procedure that can achieve good functional and cosmetic results for lower eyelid greater than 50% defects resulting from trauma or cancer excision.
It involves a tarsoconjunctival advancement flap to recreate the lower lid posterior lamella.
The anterior lamella is recreated using a full-thickness skin graft or a local skin flap.1
The Cutler-Beard flap is a cutaneoconjunctival advancement flap from the lower lid that is used for very large (greater than 70%) defects in the upper eyelid.
Indications are tumor resection, trauma, and congenital defects.
The goal is to provide lid apposition to protect the eye, good aesthetic quality, and good mobility.2
ANATOMY
The upper and lower eyelids meet at the medial and lateral canthus with the lateral canthus sitting 2 to 4 mm higher than the medial (FIG 1).
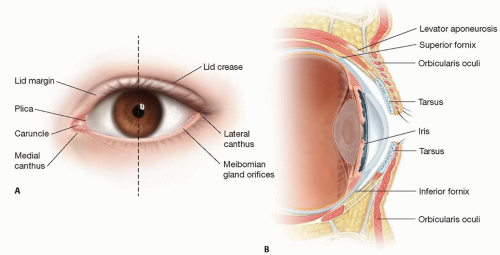
FIG 1 • A,B. External and sagittal section depicting the eyelid anatomy as well as surrounding structures.
The palpebral fissure is approximately 28 to 30 mm in length and 9 to 10 mm in height.
The eyelid anatomy can be divided into anterior and posterior lamellae.
The anterior lamella consists of the skin and the orbicularis oculi muscle.
The eyelid skin is the thinnest in the body (lesser than 1 mm). The epidermis receives its nourishment from a deeper connective tissue layer as it lacks blood vessels and lymphatics. There is a sparse amount of fat in the preseptal and preorbital skin, and fat is absent in the pretarsal skin.
The orbicularis oculi is loosely adherent to the skin and divided into orbital and palpebral portions. The palpebral is further divided into pretarsal and preseptal. The palpebral portion functions in blinking and voluntary winking. The orbital portion is for forced closure.
The posterior lamella consists of the tarsus and the conjunctiva.
The tarsal plate is composed of dense fibrous tissue. It is approximately 1 mm thick and provides the structural support of the eyelid. The upper eyelid tarsus extends from the punctum to the lateral canthus and is 30 mm long and 7 to 10 mm high, with the highest portion being centrally. The lower tarsus is only 3.8 mm wide. The ciliary border contains meibomian gland orifices that provide
the lipid layer of the tear film. The medial and lateral ends are attached to the orbital rim by the medial and lateral palpebral ligaments.
The conjunctiva is a mucous membrane that covers the sclera and the inner eyelids. The palpebral conjunctiva is adherent to the tarsus and then continues as the orbital conjunctiva where there is a plane that allows dissection from the Mueller muscle. At the fornix, the conjunctiva reflects anteriorly to become the bulbar conjunctiva.
Upper eyelid retractors
The levator palpebrae superioris arises at the orbital apex and courses anteriorly for 40 mm ending in the aponeurosis 10 mm behind the septum. At this junction, it changes direction to vertical and then inserts inferiorly onto the lower third of the tarsal plate. In addition, some fibers pass anteriorly to form the eyelid crease.
The Mueller muscle originates from the undersurface of the levator at the muscular aponeurotic junction and then travels between the levator and the conjunctiva to insert on the superior border of the tarsus. It is innervated by the sympathetic nervous system.
The lower eyelid retractors are an extension of the inferior rectus muscle.
They pass anteriorly and envelop the inferior oblique before joining the inferior transverse ligament to become the capsulopalpebral fascia and inserting at the inferior border of the tarsal plate.
A small portion of the retractors joins with Tenon capsule at the inferior fornix and courses anteriorly to form the lower lid crease.
Blood supply is derived from both the internal and external carotid arteries.
Medially, two palpebral branches (superior and inferior marginal arteries) arise from the ophthalmic to supply the upper and lower lid. These arteries then travel horizontally as the marginal arcades that lie on the tarsal plate (4 mm from the upper margin and 2 mm from the lower margin).
Laterally, the lacrimal artery provides branches to both the upper and lower lids, which travel horizontally to anastomose with the marginal arcades.
The external carotid contributes through branches of the facial, superficial temporal, and infraorbital arteries.
PATIENT HISTORY AND PHYSICAL FINDINGS
The preoperative evaluation includes a detailed examination of the extent of the lid defect, in particular, the extent of involvement of the anterior and posterior lamellae.
The adjacent skin, contralateral upper eyelid, postauricular, and supraclavicular areas should be inspected for potential donor skin.
IMAGING
Preoperative photos should be taken to document the extent of the defect.
Imaging with CT or MRI can be considered based on etiology of the defect, in particular in trauma situations to assess other injuries or embedded foreign body.
SURGICAL MANAGEMENT
Preoperative Planning
In determining whether a Hughes procedure is appropriate, one must consider the size and location of the defect as well as the status of the other eye.
An alternative procedure may be preferred if there is limited vision in the opposite eye as vision will be temporarily obscured by the vascular flap.
The extent of the posterior lamella defect and the anterior lamella defect must be determined to assess the size the flap as well as to determine the donor site for the skin graft.
The extent of the posterior lamella defect and the anterior lamella defect must be determined to assess the size of the Cutler-Beard flap.
It is also important to assess the visual function of the contralateral eye as this procedure requires closure of the eye for up to 3 weeks.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree