Introduction
The nose is located in the center of the face and is one of the most impressive features to other people. The shape is a three-dimensionally complex and differs between individual, sex, and race. This complex structure is formed by skin, soft tissue, bone, cartilage, and mucosa, which differ in composition depending on the region of the nose. The vascular supply and innervation of the nose are also intricate. Several vessels and nerves are distributed within the relatively small space of the nose. Thus, it is essential to have a good understanding of the anatomy of the nose for any surgical procedure.
External Anatomy of the Nose
In the lateral view of the skeleton, the uppermost part of the nasal bone connects to the frontal bone by the nasofrontal suture. The midline point on the suture is defined as the nasion. The depressed area below the nasion is the nasal root, where the most depressed part is usually located slightly superior to the medial canthal tendon of the eyelid. On the skin, the most depressed point is usually more cranial to the point directly over the bony nasal root because the subcutaneous fat and the mimetic muscles are thick in this area. Heading downward along the nasal ridge, the long straight part protruding anteriorly is the nasal dorsum. The nasal dorsum is narrowest at the intercanthal line, which is the line connecting the bilateral medial canthal tendons that becomes wider as you move down the nose. The junctional point between the upper lateral cartilage and lower lateral cartilage is the supratip breakpoint, which is the inferior border of the nasal dorsum. Below the supratip break point, the highest part of the nose is the nasal tip, and the highest point is the pronasale. The inferior border of the nasal tip is the columellar breakpoint, which is the point corresponding to the angle between the medial crus and middle crus of the lower lateral cartilage. The area superior to the tip defining point in the nasal tip is the supratip lobule and inferior to the point is the infratip lobule. The columella is the inferior margin of the nasal septum, ending in the subnasale (Fig. 17.1).
In the inferior view, the shape of the nostril and the length of the columella affect the general shape of the lower nose. In general, the length between the bilateral alar creases and the length from the subnasale to the pronasale are equal. Furthermore, the ratio between the length of the height of the nostril and the length of the infratip lobule is 2:11; however, the shape and proportion of this area vary by race (Fig. 17.2).2,3
Skin
The characteristics of the nasal skin are distinctly different between its upper and lower parts. The upper part of the skin tends to be thin and mobile. Some wrinkles can be observed during changes in facial expression. Conversely, the skin in the lower part of the nose is thicker and tends to fix to underlying structures. As a result, wrinkles are not observed during changes in facial expression in this area. The skin also plays a role in forming the three-dimensionally complicated nasal structure with the underlying cartilage. The lower part of the skin usually has many exocrine glands, namely, sebaceous and sweat glands. Regarding the thickness of the nasal skin, Lesserd and Daniel reported that it is thickest at the nasofrontal groove at approximately 1.25 mm and thinnest at the rhinion at approximately 0.6 mm.1,4 This means that the skin is the thinnest in the middle area of the nose (around the rhinion), and becomes thicker above and below this point. The thickness of the skin changes by region with the skin in the columella and along the alar margin usually being thinner.1 At the nostril apex, there is a soft triangle where the nostril lining skin and lobule skin touch without any subcutaneous structure (Fig. 17.2).
Subcutaneous Layer
Lesserd and Daniel also reported that four layers are observed in the soft tissue structures under the skin: the superficial fatty panniculus; the fibromuscular layer; the deep fatty layer; and the periosteum (or perichondrium) (Fig. 17.3). The superficial fatty panniculus is the layer consisting of subdermal adipose tissue and interlacing vertical fibrous septa. This layer presents throughout the nose but is concentrated in the glabellar and supratip regions. The fibromuscular layer consists of nasal muscles and fibrous layers covering the muscles from superficial and deep aspects. This layer is defined as the nasal superficial musculoaponeurotic system (SMAS) and is continuous with the facial SMAS. The deep fatty layer consists of the loose areolar fat without fibrous septa, which gives mobility to nasal skin.5
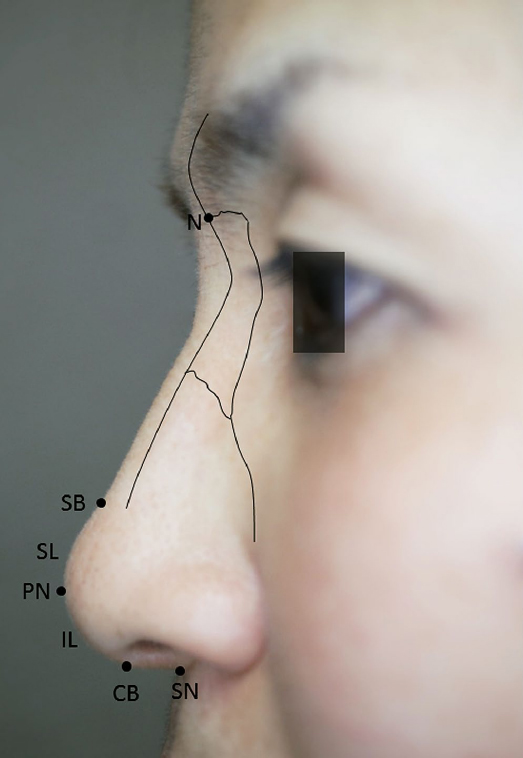
Fig. 17.1 The lateral view of the external nose. CB, Columella break-point; IL, infratip lobule; N, nasion; PN, pronasale; SB, supratip breakpoint; SL, supratip lobule; SN, subnasale.
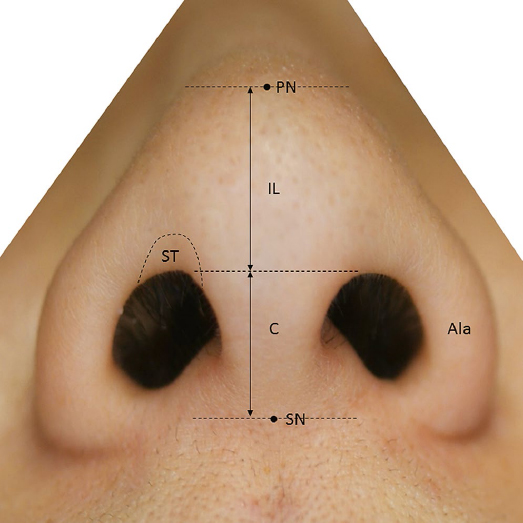
Fig. 17.2 The inferior view of the external nose. C, Columella; IL, infratip lobule; PN, pronasale; SN, subnasale; ST, soft triangle.
Muscle Layer of the Nose
The musculature of the nose is categorized functionally into four groups: the elevators; depressors; compressors; and dilators (Table 17.1).1,4,6 The elevators include the procerus, levator labii superioris alaeque nasi, and anomalus nasi muscles. These muscles have a role in lifting and shortening the nose, and also in opening the nasal valve. The depressors include the alar part of the nasalis muscle and depressor septi muscle. These muscles lengthen the nose and dilate the nostril. The compressor includes the transverse part of the nasalis muscle. This muscle also works to lengthen the nose and narrow the nostril. The dilators consist of the dilator naris anterior and posterior muscles and work to dilate the nostril. The zygomatic branch of the facial nerve innervates each of these muscles.
Blood Supply of the Nose
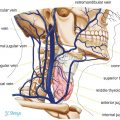
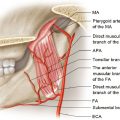
Four arteries originating either from the internal carotid or from the external carotid arteries are the main supply for the external nose (Table 17.2). The arteries originating from the internal carotid artery are the dorsal nasal and anterior ethmoidal arteries, both of which are branches of the ophthalmic artery. Two arteries, the angular artery and superior labial artery, originate from the facial artery, one of the main branches of the external carotid artery.
The dorsal nasal artery emerges from the orbital cavity to the subcutaneous layer above the medial canthal tendon, which runs obliquely inferomedially and distributes in the upper dorsal part of the nose. The anterior ethmoidal artery, which is also a branch of the ophthalmic artery, emerges from the base between the nasal bone and the lateral nasal cartilage and runs downward to the nasal tip. The angular artery, which is a continuation of the facial artery, has a number of branches, such as the lateral nasal branch to the lower lateral nose. The superior labial artery primarily supplies the nostril sill and columella.
The venous drainage of the nose is carried out by veins with the same name as the arteries they travel with. These finally drain into the facial vein or the cavernous sinus via the ophthalmic vein.
The arterial and venous networks distribute in or above the mimetic muscle layer (fibromuscular layer; nasal SMAS layer). Then, the desirable layer of dissection of the nose is under the fibromuscular layer to preserve the blood circulation of the nasal skin, prevent bleeding, and to reduce edema after surgery. Especially, open rhinoplasty requires extremely accurate treatment about dissection of the layers.
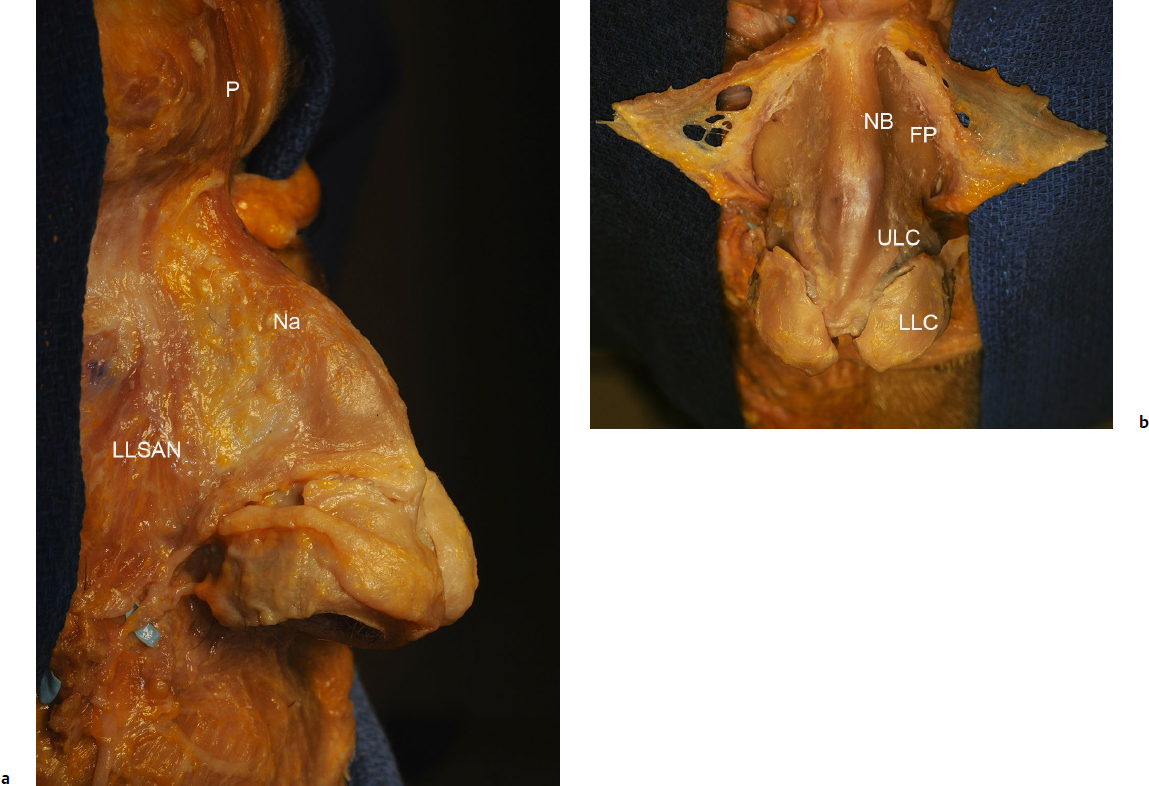
Table 17.1 Muscles of the nose
Group | Action | Muscles |
Elevators | Lifting and shortening the nose | Procerus |
Depressors | Lengthening the nose and dilating the nostril | Alar part of the nasalis |
Compressors | Narrowing the nostril | Transverse part of the nasalis |
Dilators | Dilating the nostril | Dilator naris anterior and posterior |
Table 17.2 Blood supply of the nose
Artery | Origin | Distribution |
Dorsal nasal artery | Ophthalmic artery | Upper dorsal part |
Anterior ethmoidal artery | Ophthalmic artery | Nasal tip |
Branches of the angular artery | Facial artery | Lower lateral nose |
Superior labial artery | Facial artery | Nostril and columella |
Table 17.3 Sensory innervation of the nose
Nerve | Origin | Distribution |
Supratrochlear nerve | Ophthalmic nerve | Upper part of the nose |
Infratrochlear nerve | Ophthalmic nerve | Upper part of the nose |
Anterior ethmoidal nerve | Ophthalmic nerve | Distal dorsum and nasal tip |
Infraorbital nerve | Maxillary nerve | Distal nose (ala, columella, etc.) |
Sensory Innervation of the Nose
Four nerves, the supratrochlear, the infratrochlear, the anterior ethmoidal, and the infraorbital nerves provide sensory innervation to the external nose (Table 17.3). The supratrochlear and infratrochlear nerves originate from the ophthalmic division of the trigeminal nerve, emerging from the medial orbital rim and traveling to the subcutaneous layer to be distributed to the upper part of the nose. The anterior ethmoidal nerve emerges from between the nasal bone and lateral nasal cartilage, and is distributed to the distal dorsum and the nasal tip. Injury of the anterior ethmoidal nerve causes sensory disturbance to the nasal tip. The infraorbital nerve is a branch of the maxillary division of the trigeminal nerve that runs inferomedially to the ala after emerging from the infraorbital foramen, and distributes in the distal nose, including the ala and columella.
Bony and Cartilaginous Structures of the Nose
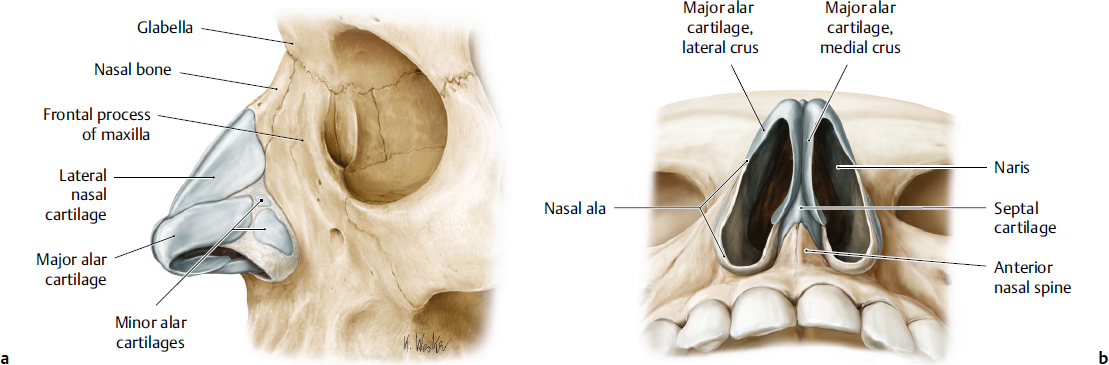
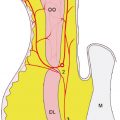
The bony and cartilaginous frame of the nose can be divided into three parts according to structure (Fig. 17.4). Pairs of nasal bones form the upper part and frontal processes of the maxilla, the middle part is made of pairs of upper lateral cartilages, and the lower part consists of lower lateral cartilages.
In the upper part, the paired nasal bones and frontal processes of the maxilla form the pyramidal vault in horizontal section. The paired nasal bones are rectangular shaped bone and fuse in the midline. In the lateral view, the nasal bone changes the angle of the ridgeline at approximately the upper one-third point, defined as the nasofrontal groove. The nasal bone is also fused with the frontal bone superiorly by the frontonasal suture and with the frontal process of the maxilla by the nasomaxillary suture. The inferior border joins to the upper lateral cartilage. At the internal surface, the nasal bone connects with the structures forming the nasal septum, such as the nasal spine of the frontal bone, the perpendicular plate of the ethmoid, and the cartilage of the nasal septum. The nasal bone is generally thicker and narrower in the superior region and thinner and wider inferiorly. The bone varies in form and size in different individuals. However, Lessard and Daniel reported that the average length from the nasofrontal suture line to the inferior border is 25.1 mm.4 The frontal process of the maxilla is the upward projection of the maxilla and fuses with the frontal bone superiorly, with the nasal bone medially, and the lacrimal bone laterally. The levator labii superioris alaeque nasi and orbicularis oculi muscles attach to the process. The medial canthal tendon attaches to the frontal process at the narrowest part of the nose. The line connecting the bilateral medial canthal tendona is the intercanthus line. Taking the inter canthus line as a reference, the nasofrontal suture is ~10.7 mm above, the nasofrontal groove is ~5.8 mm above, and the inferior border of the nasal bone is ~14.4 mm below the line.4
In the middle part of the nose, the upper lateral cartilage makes up the hard structure. At the transition zone between the nasal bone and upper lateral cartilage, nasal bone overlaps the cartilage (the nasal bone lies on the upper lateral cartilage), and they connect to each other by dense connective tissue. The overlapping area is called the keystone area, which forms a crescent shape in a concave upward direction, widest in the midline, decreasing in width laterally.7 In the upper region of the upper lateral cartilage, including an overlapping area, the bilateral upper lateral cartilages and the cartilaginous part of the nasal septum integrate as a unified structure, but a linear gap appears between the upper lateral cartilage and the septal cartilage that constitutes less than two-thirds of the area (Fig. 17.5). Some people consider the upper lateral cartilages to be winglike extensions of the septal cartilage.8–10 At the lowest part, the upper lateral cartilage connects with the lateral crus of the lower lateral cartilage, which is referred to as the scroll.9 In most cases, these two cartilages overlap in various shapes, and this connection bears a major tip-supporting mechanism.11
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


