Excision of Soft Tissue Tumors of the Lower Leg
Raffi S. Avedian
Robert J. Steffner
DEFINITION
Soft tissue tumors of the lower leg may be benign or malignant (soft tissue sarcoma) and exhibit a variable natural history ranging from latency to rapid growth.
Tumors located entirely above the muscle fascia are considered superficial, whereas tumors involving the fascia or deep to it are considered deep.
ANATOMY
The lower leg is made up of the tibia and fibula and four muscle compartments: anterior, lateral, deep posterior, and superficial posterior (FIG 1).
Three principal arteries travel in the lower leg.
The posterior tibial artery is located in the deep posterior compartment on the surface of the tibialis posterior.
The anterior tibial artery is in the anterior compartment located deep to the muscles on the surface of the interosseous membrane.
The fibular artery travels in the deep posterior compartment medial to the fibula under the flexor hallucis longus; it sends branches to the lateral and anterior compartments and a nutrient vessel to the fibula.
The deep peroneal nerve travels with the anterior tibial artery. The superficial peroneal nerve is located in the lateral compartment; in the distal one-third of the leg, it travels between the peroneus muscles and extensor digitorum longus and pierces the deep fascia to become a cutaneous nerve.
PATHOGENESIS
The mechanism for soft tissue tumor formation is not known.
Risk factors for sarcoma development include radiation exposure, radiotherapy, pesticide exposure, and hereditary conditions including Li-Fraumeni syndrome and retinoblastoma gene mutation.
NATURAL HISTORY
All soft tissue sarcomas have the potential for local recurrence and metastasis.1
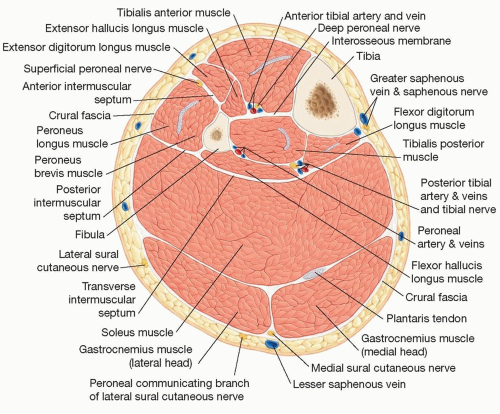
FIG 1 • Cross-sectional anatomy of lower leg showing the contents of the anterior, lateral, superficial posterior, and deep posterior compartments.
Soft tissue sarcomas exhibit a spectrum of natural history from slow-growing low-grade tumors with low risk of metastasis to high-grade sarcoma that may grow rapidly and pose a high risk of metastasis.
Lungs are the most common site of metastasis. Lymph node involvement is rare.
Angiosarcoma, clear cell sarcoma, epithelioid sarcoma, rhabdomyosarcoma, myxofibrosarcoma, and synovial sarcoma are associated with increased risk of lymph node spread compared to other sarcomas.2
Benign tumors by definition do not have metastatic potential but can grow to large sizes and cause symptoms.
PATIENT HISTORY AND PHYSICAL FINDINGS
A thorough history and examination are important to assess duration of symptoms, comorbidities, physical dysfunction, organ involvement, overall health, and patient expectations in order to best tailor treatment strategy for the individual patient.
Many sarcomas may be asymptomatic with the only patient complaint being the presence of a mass.
Neurovascular examination is mandatory for any extremity tumor.
IMAGING
Magnetic resonance imaging is the principal imaging modality used to characterize tumors, formulate differential diagnosis, define local tissue infiltration, and formulate surgical plan.
Plain radiographs are used if there is concern for bone involvement or to demonstrate mineralization within a tumor such as vascular malformations.Related posts:
 Fasciotomy of the Thigh, Lower Leg, and Foot
Fasciotomy of the Thigh, Lower Leg, and Foot
 Bony Reconstruction of Foot and Ankle (Bone Grafts)
Bony Reconstruction of Foot and Ankle (Bone Grafts)
 Vascular Reconstruction of Lower Extremity, Foot, and Ankle
Vascular Reconstruction of Lower Extremity, Foot, and Ankle
 Soft Tissue Coverage of Lower Leg—Soleus Flap
Soft Tissue Coverage of Lower Leg—Soleus Flap
 Reconstruction of Femur
Reconstruction of Femur
 Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation
Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


