Excision of Bone Tumors of the Lower Leg
Raffi S. Avedian
Rohit Khosla
DEFINITION
Bone tumors of the tibia and fibula may be benign or malignant (bone sarcoma) and exhibit a variable natural history ranging from latent to rapid growth. Aggressive benign tumors and malignant tumors typically cause pain, dysfunction, and fracture.
A bone tumor located in the tibia or fibula such that definitive treatment requires excision of an intercalary segment of bone, sparing the ankle and knee joints, is discussed in this chapter.
ANATOMY
The lower leg is made up of the tibia and fibula and four muscle compartments: anterior, lateral, deep posterior, and superficial posterior (FIG 1).
Three principal arteries travel in the lower leg. The posterior tibial artery is located in the deep posterior compartment on the surface of the tibialis posterior. The anterior tibial artery is in the anterior compartment located deep to the muscles on the surface of the interosseous membrane. The fibular artery travels in the deep posterior compartment medial to the fibula under the flexor hallucis longus; it sends branches to the lateral and anterior compartments and a nutrient vessel to the fibula.
The deep peroneal nerve travels with the anterior tibial artery. The superficial peroneal nerve is located in the lateral compartment; in the distal one-third of the leg, it travels between the peroneus muscles and extensor digitorum longus and pierces the deep fascia to become a cutaneous nerve.
PATHOGENESIS
The mechanism for bone tumor formation is not known.
Risk factors for sarcoma development include radiation exposure, radiotherapy, pesticide exposure, and hereditary conditions including Li-Fraumeni syndrome and retinoblastoma gene mutation.
NATURAL HISTORY
Active benign tumors such as giant cell tumor of bone, chondroblastoma, and aneurysmal bone cyst will progress over time and may recur after excision but are not lethal.
All bone sarcomas have the potential for local recurrence and metastasis.
Some bone sarcomas such as low-grade chondrosarcoma exhibit a slow rate of growth and low risk of metastasis, whereas aggressive tumors like high-grade osteosarcoma and dedifferentiated chondrosarcoma grow rapidly and have a relatively high risk of metastasis.
Tumor variables that are associated with increased risk of metastasis include high grade and large size (greater than 8 cm).
Lungs and other osseous sites are the most and second most common location of metastasis, respectively.
PATIENT HISTORY AND PHYSICAL FINDINGS
Pain is a common presenting symptom for aggressive bone tumors.
A thorough history and examination are important to assess duration of symptoms, comorbidities, physical dysfunction, organ involvement, overall health, and patient expectations to best tailor treatment strategy for the individual patient.
Neurovascular examination is mandatory for any extremity tumor.
IMAGING
Plain radiographs are used to formulate a differential diagnosis and a preoperative plan.
Magnetic resonance imaging is routinely used to determine the extent of intramedullary tumor involvement, presence of soft tissue extension, status of the neurovascular structures, and preoperative planning.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis for a bone tumor includes benign tumors, sarcomas, lymphoma of bone, infection, and metabolic lesions (eg, hyperparathyroidism).
The most common bone sarcomas are osteosarcoma, chondrosarcoma, and Ewing sarcoma.
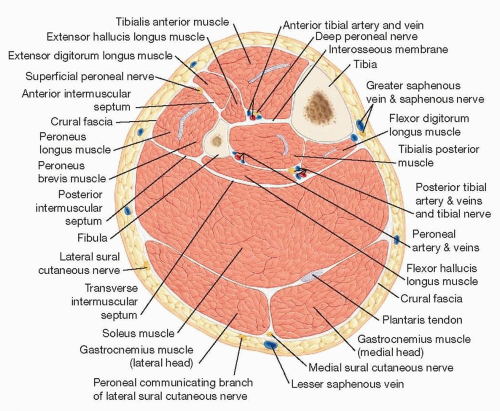 FIG 1 • Cross-sectional anatomy of the lower leg showing the contents of the anterior, lateral, superficial posterior, and deep posterior compartments. |
SURGICAL MANAGEMENT
The appropriate treatment for any musculoskeletal tumor is based on its diagnosis and natural history.
Biopsy incisions are considered contaminated and must be resected at the time of definitive surgery. Care should be taken to place the biopsy in a location that does not interfere with the final surgical plan.
Intralesional curettage is the preferred treatment for benign tumors. Radical resection with a clean margin is required for bone sarcomas.
Reconstruction depends on the extent of bone excision and may include simple bone grafting, endoprosthetic implants, structural allografts, vascularized fibula (ipsilateral centralized or contralateral free transplant), or combined allograft and vascularized fibula.
The goal of surgery is to remove the tumor adequately to minimize recurrence and restore the mechanical integrity of the bone and joints so that the patient may have sufficient function to perform activities of daily living with minimal pain.
Preoperative Planning
A patient is considered ready for surgery after completion of staging and multidisciplinary review of pertinent imaging, pathology, and treatment strategy.
The surgical plan is created by thorough study of the preoperative radiographs and MR imaging.
Bone cuts are planned by measuring on preoperative imaging the distance from an intraoperatively identifiable landmark (eg, medial malleolus or tibial condyle) to the desired osteotomy site (FIG 2A,B).Related posts:
 Fasciotomy of the Thigh, Lower Leg, and Foot
Fasciotomy of the Thigh, Lower Leg, and Foot
 Bony Reconstruction of Foot and Ankle (Bone Grafts)
Bony Reconstruction of Foot and Ankle (Bone Grafts)
 Vascular Reconstruction of Lower Extremity, Foot, and Ankle
Vascular Reconstruction of Lower Extremity, Foot, and Ankle
 Soft Tissue Coverage of Lower Leg—Soleus Flap
Soft Tissue Coverage of Lower Leg—Soleus Flap
 Reconstruction of Femur
Reconstruction of Femur
 Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation
Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


