Erector Spinae (Paraspinous) Muscle Flap
Lauren M. Mioton
Gregory A. Dumanian
DEFINITION
The erector spinae muscle flap is used for coverage of spinal wounds.
ANATOMY
The erector spinae, also known as the paraspinous muscles, are paired structures comprised of the iliocostalis (most medial), longissimus, and spinalis muscles (most lateral).
The iliocostalis muscle originates from the sacrum, erector spinae aponeurosis, and iliac crest, with insertions onto the ribs and transverse processes of C6-C4. It contributes to extension and lateral flexion of the vertebral column.
The longissimus muscle is the largest of the erector spinae with varying portions originating from the sacrum and transverse processes of the lumbar and thoracic vertebra. It inserts into the transverse processes of lumbar, thoracic, and cervical vertebrae. It contributes to extension and lateral flexion of the vertebral column.
The spinalis muscle originates from and inserts into the spinous process of lumbar and thoracic vertebrae. It aids with extension of the vertebral column.
The erector spinae muscles are round and large along the inferior aspect of the lumbar region but become thinner more superiorly along the underside of the trapezius.
They have a convex shape with segmental blood vessels originating from the thoracic and abdominal aorta, entering on the lateral and deep aspects of the longissimus and iliocostalis muscles. There are typically both lateral and medial vessels entering the erector spinae, and all of the muscle will stay viable just on its lateral blood flow. In the thorax, these vessels travel through the lateral border of the erector spinae to be the minor pedicle of the latissimus muscle.
PATIENT HISTORY AND PHYSICAL FINDINGS
Past medical and surgical history with attention to the back is necessary. Prior spine incisions, their location, a history of radiation, and a history of prior infections should be sought. A focused physical examination documenting prior incisions and the suppleness of the posterior soft tissues should be performed. A history of spina bifida, a cord lipoma, or lack of fusion of the posterior spinal tube implies a lack of development and/or small size of the erector spinae inferiorly.
A prior, or planned, lateral approach to the spine may lead to transection of the erector spinae muscles and eliminate it as a flap option.
IMAGING
No preoperative imaging is warranted in preparation for this flap.
SURGICAL MANAGEMENT
The erector spinae muscles are no longer functional for spine extension and flexion and seen as expendable following spine fusion.
It is an appropriate flap for wounds ranging from the high cervical to low lumbar region.
It may not provide coverage of high occipital or the sacral recess (between the sacrum and lumbar spine).
Preoperative Planning
The patient’s medical history should be reviewed as prior to any planned surgery.
Positioning
The patient is placed in the prone position for the erector spinae flap procedure. Arms may be tucked at the patient’s side or abducted with elbows at 90 degrees.
Approach
The spinal wound, especially if chronic in nature, should be appropriately excised and debrided prior to reconstruction.
Patients who have undergone prior spine surgery may have notable scar tissue in the wound bed. Clearing the surgical bed of this fibrous tissue will reduce the likelihood of postoperative wound complications as well as allow the surgeon to properly identify the erector spinae muscles and dissection planes.
Spinal closures are performed prophylactically after spine instrumentation to help achieve a durable closure (especially after multiple prior surgeries) and also for treatment of acute postoperative spinal hardware infections. In the latter, the hardware should be assessed for stability and maintained if it feels stable. Switching out of components of the hardware and rendering it less prominent is at the discretion of the spine team. Loose nonincorporated bone graft should be removed, but it is not necessary to remove every piece of bone graft.
TECHNIQUES
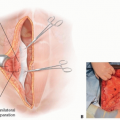
▪ Erector Spinae Muscle Flap
Skin flaps are elevated on either side of the wound either deep or superficial to the thoracolumbar fascia, allowing the latissimus and trapezius muscles to stay attached to the skin.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree