Epidermolysis bullosa (EB) has officially been recognized as a rare disease in Italy. Regional reference centers for EB have been created during the past years. This article discusses the clinical services and coordinated multidisciplinary management of EB in Italy.
In 2001, the Italian Ministry of Health issued a law for the creation of a national network of reference centers for the diagnosis and care of rare diseases, defined as diseases with a prevalence of less than 5:10,000. According to this law, reference centers for rare diseases are identified on a regional basis and are charged to (1) assure disease diagnosis, (2) release a specific certification to the patient, (3) ensure proper management and follow-up—also through collaboration with general practitioners, (4) keep patients’ records and communicate all new disease cases to a regional registry for rare diseases, (5) organize training of health care personnel, (6) disseminate information and raise public awareness about rare diseases, and (7) keep contacts with patients’ associations. The coordination of epidemiologic, clinical, and research activities on rare diseases, including the collection of epidemiologic data from regional registries and their organization in a national registry and the release of guidelines for disease diagnosis and care, is assigned to the National Institute of Health where a National Center for Rare Diseases (NCRD) has been created. According to this law, the National Health System covers costs related to (1) examinations required to establish the disease diagnosis, including molecular diagnosis and prenatal diagnosis; (2) laboratory examinations, specialists’ consultations, and hospitalization; and (3) drugs. Other items that can be paid by the National Health System include medical devices and antiseptics, emollients, dietary supplements, dressings, etc.
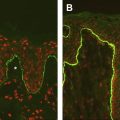
As inherited epidermolysis bullosa (EB) is officially recognized as a rare disease in Italy, regional reference centers for EB have been created during the past years (the reference center list is available at the NCRD Web site: http://www.iss.it/cnmr/ ). These centers provide clinical services for patient primary care. In addition, coordinated multidisciplinary management is offered in some centers. In particular, the Pediatric Hospital Bambino Gesù in Rome has organized an outpatient clinic under the coordination of the Dermatology Unit where the patients are offered a wide range of medical specialties (dermatology, pediatrics, gastroenterologic and plastic surgery, anesthesiology, ophthalmology, dentistry, otorhinolaryngology, orthopedics, cardiology, nephrology, psychology, etc) according to the individual’s needs. As for EB diagnosis, centers that perform both immunofluorescence antigen mapping and ultrastructural analysis include the Center for Inherited Skin diseases of the Institute of Dermatologic Sciences in Milan and the authors’ laboratory (Laboratory of Molecular and Cell Biology, IDI-IRCCS) in Rome. Molecular testing for EB is assured by two centers: the Division of Biology and Genetics, Department of Biomedical Sciences and Biotechnology, University of Brescia, where the COL7A1 gene is screened and the authors’ laboratory in Rome, where about 200 molecular diagnoses for various EB types have been performed in the last years. In particular, the genotyping of Italian patients with recessive dystrophic EB (RDEB) (89 cases), Herlitz junctional EB (HJEB) (20 cases), and Kindler syndrome (KS) (17 cases) has led to the identification of a number of recurrent mutations in the causative genes ( Table 1 ). The majority of these variants were detected in families from specific Italian regions and haplotype analysis of highly polymorphic intragenic single nucleotide polymorphisms or flanking polymorphic microsatellites in the patients carrying these mutations indicated a common ancestral origin for the corresponding mutant allele. At present, seven frequent mutations in COL7A1 cover the 34% of the RDEB alleles, eight mutations (four in LAMB3 and three in LAMC2) target the 62.5% of the mutant HJEB alleles, and four recurrent FERMT1 mutations comprise the 73.5% of Italian KS alleles (see Table 1 ). These findings have allowed the optimization of priority strategies for mutation detection in new Italian patients with EB.
| Mutation | Number of Mutated Alleles | Percent of Mutated Alleles | Geographic Origin | Detection Method |
|---|---|---|---|---|
| COL7A1 | ||||
| c.497insA | 21 | 11.8 | Widespread | Sequencing |
| c.4783-1G>A | 6 | 3.4 | Sicily | Sequencing |
| c.7344G>A | 10 | 5.6 | Widespread | HphI |
| c.425A>G | 6 | 3.4 | Widespread | StyI |
| p.G1664A | 6 | 3.4 | Apulia | PstI |
| c.8441-14del21 | 7 | 3.9 | Sicily | Sequencing |
| c.8074delG | 5 | 2.8 | Apulia | Sequencing |
| LAMB3 | ||||
| p.R635X | 3 | 7.5 | Widespread | Bgl II |
| p.R81X | 3 | 7.5 | Widespread | Sequencing |
| p.W143X | 4 | 10.0 | Campania | Bst NI |
| c.31insC | 4 | 10.0 | Widespread | Sequencing |
| LAMC2 | ||||
| p.R95X | 4 | 10.0 | Sicily | Taq I |
| p.Y355X | 4 | 10.0 | Calabria | Sequencing |
| p.R223X | 3 | 7.5 | Sicily | Sequencing |
| FERMT1/KIND1 | ||||
| c.373delT | 4 | 11.8 | Central Italy | Sequencing |
| c.1161delA | 6 | 17.6 | Central Italy | Sequencing |
| g.70250_74168del | 9 | 26.5 | Calabria | PCR |
| c.958-1G>A | 6 | 17.6 | Central Italy | Sequencing |
Related posts:
 How to Take Skin Biopsies for Epidermolysis Bullosa
How to Take Skin Biopsies for Epidermolysis Bullosa
 Epidermolysis Bullosa Simplex with Muscular Dystrophy
Dilated Cardiomyopathy in Epidermolysis Bullosa
Bone Marrow Stem Cell Therapy for Recessive Dystrophic Epidermolysis Bullosa
Epidermolysis Bullosa Simplex with Muscular Dystrophy
Dilated Cardiomyopathy in Epidermolysis Bullosa
Bone Marrow Stem Cell Therapy for Recessive Dystrophic Epidermolysis Bullosa
 Epidermolysis Bullosa in France: Management in the National Reference Center for Genodermatosis
Epidermolysis Bullosa Care in Israel
Epidermolysis Bullosa in France: Management in the National Reference Center for Genodermatosis
Epidermolysis Bullosa Care in Israel
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


