| Recurrent corneal abrasions, keratitis or infections |
| Corneal scarring |
| Visual impairment secondary to corneal compromise or astigmatism |
| Assess for degree of anterior lamellar redundancy |
| Assess for eyelash-corneal touch and horizontal extent of eyelid eversion |
| Assessment of the effects of astigmatism and corneal integrity on vision |
| Corneal staining with fluorescein to detect epithelial defects, irregularities, and scarring |
Introduction
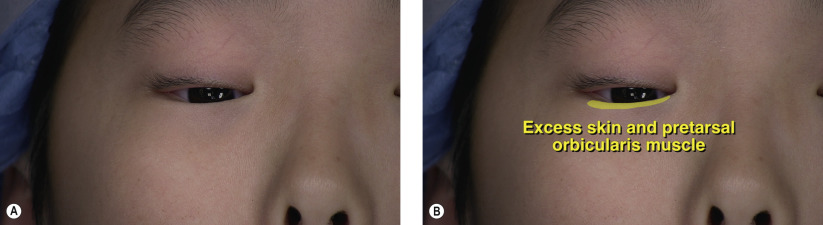
Epiblepharon is an eyelid condition in which excess orbicularis muscle and skin override the upper or lower eyelid margin. The etiology of this congenital anomaly is likely due to inadequate lower eyelid retractor development, where there is a lack of fenestrating fibers from the retractor aponeurosis which inserts under the skin. It can also be secondary to pretarsal orbicularis muscle that inserts abnormally close to the eyelid margin. This condition exhibits a familial tendency in an autosomal dominant pattern and can also present in patients with prominent cheeks. Found most commonly in Asian and Hispanic infants due to nasal bones that elevate at a later age, epiblepharon typically resolves spontaneously within the first 2 years of life as the patient undergoes facial bone growth, resulting in vertical skin and muscle extension and greater tension on the retractors.
In the evaluation of patients with epiblepharon, a history of tearing, photophobia, chronic ocular irritation, eye rubbing, and mucous discharge is commonly elicited. The patient may report tearing or a constantly wet and mattered eye. Symptoms may be exacerbated in downgaze, which maximizes ciliary-corneal contact. Decreased visual acuity with significant astigmatism may be present as a consequence of frequent eyelid squeezing or rubbing in response to foreign body sensation. The eyelid and margin exam will reveal a redundant fold of eyelid skin and underlying orbicularis present bilaterally, typically involving the medial one-third to one-half of the upper or lower eyelid. This prominent fold may result in the vertical misdirection of a few or many cilia towards the ocular surface, especially along the nasal half of the lower eyelid. A slit-lamp biomicroscopic examination is performed to determine if the eyelashes are rubbing against the conjunctiva or cornea. Signs of keratitis include conjunctival injection, epithelial defects that stain with fluorescein dye, corneal infiltrates, and corneal neovascularization.
Patients usually tolerate this condition well and treatment is only necessary if the eyes become inflamed or irritated. Since the eyelashes are fine and soft, the cornea typically responds to ocular lubricants in most cases. Patients need regular follow-up for surveillance and treatment for corneal and conjunctival irritation and abrasions. If left untreated, the long-term sequelae of chronic ocular irritation secondary to epiblepharon can range from corneal punctate erosions in mild cases to keratitis, infection, and permanent scarring in severe cases.
Although this condition usually resolves spontaneously, surgical intervention is indicated in patients who experience significant corneal involvement or visual compromise. The underlying principle of surgical correction is to effect an external rotation of the cilia away from the globe. The placement of full thickness everting sutures is a simple and quick method of everting the eyelid. However, since this method of repair is associated with occasional suture infections and a high recurrence rate, it is considered a temporizing rather than a definitive measure. Our preferred approach is removal of the excess anterior lamellae and placement of eyelid rotational sutures from the orbicularis to the distal tarsal border. Epicanthal folds may be associated with epiblepharon and correction, if desired, can be performed concurrently with a medial epicanthoplasty as described in Chapter 7 . Surgical correction of epiblepharon is associated with a high success rate but may infrequently lead to complications such as ectropion, scarring of the conjunctival cul-de-sac, and lower eyelid retraction.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


