| Cicatricial entropion with lashes abrading cornea |
| Posterior lamellar scarring with transverse cicatricial bands |
| Corneal erosions and foreign body sensation secondary to entropion |
| Assess posterior lamella with eyelid eversion; look for transverse horizontal bands |
| Assess eyelid laxity |
| Quantify horizontal length of eyelid involvement |
| Prior eyelid, facial surgery or trauma |
| Any history of infections, chemotherapy, topical medication use, oral ulceration |
Introduction
Cicatricial entropion caused by posterior lamellar contraction has many causes. Infectious, inflammatory, medication-induced, and autoimmune are the most common etiologies. Prior to definitive surgical repair, systemic medical control of the underlying disease is paramount. Foreign body sensation, irritation, and redness occur as the posterior aspect of the eyelid margin rotates inward. Corneal involvement with epithelial defects arises as the lashes begin to abrade the ocular surface.
For mild cicatricial entropion, anterior lamellar repositioning will typically suffice. For moderate to severe cicatricial entropion, the posterior tarsotomy is particularly effective and simply means to rotate the eyelid margin and reduce the cicatricial forces causing inversion. For severe cicatricial entropion, placement of a posterior lamellar graft such as autologous hard palate may be required.
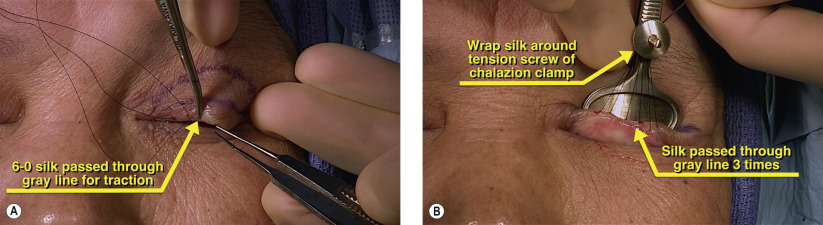
The posterior tarsotomy differs from the Wies procedure ( Chapter 30 ) in that only the tarsus is incised. A full thickness tarsal incision is made 1.5 mm from the eyelid margin within the horizontal transverse bands of the tarsus on the upper eyelid. On the lower eyelid, the incision is made 1 mm from the eyelid margin. Blunt and sharp dissection then allows the eyelid to rotate with placement of everting sutures. The tarsotomy can be tailored to the degree of horizontal involvement and it can be performed segmentally if desired. Slight overcorrection is desired, as a mild degree of inversion will gradually occur postoperatively.
Surgical Technique
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


