| Forehead rhytids |
| Moderate brow ptosis |
| Temporal hooding |
| Facial nerve palsy with brow ptosis |
| Position of brow |
| Age and gender of patient |
| Magnitude of brow ptosis |
| Location of hairline and quantity of follicles |
| Prior eyelid, facial surgery or trauma |
| Qualitative and quantitative assessment of tear film |
Introduction
The endoscopic forehead lift is primarily a cosmetic operation and is useful for moderate brow ptosis. It can smoothen out forehead rhytids, weaken brow depressors, and elevate the tail of the brow. For mild brow ptosis, an internal brow elevation can be performed ( Chapter 21 ). This procedure is most effective in preventing post-upper blepharoplasty brow descent but provides minimal brow elevation. For moderate brow ptosis where function takes precedence over form, a direct browplasty can be performed to elevate a ptotic brow ( Chapter 20 ). For more severe brow ptosis in select patients, pretrichial browplasty can be performed ( Chapter 23 ).
Critics of the endoscopic technique claim that this procedure is not as effective in lifting the brow as an open procedure and that the effects are not long lasting. However, we have found the procedure to be useful in mild-to-moderate brow ptosis with good long-term results. Furthermore, the endoscopic procedure has the advantage of resulting in less hair loss, hypesthesia, and skin scarring compared to open brow approaches.
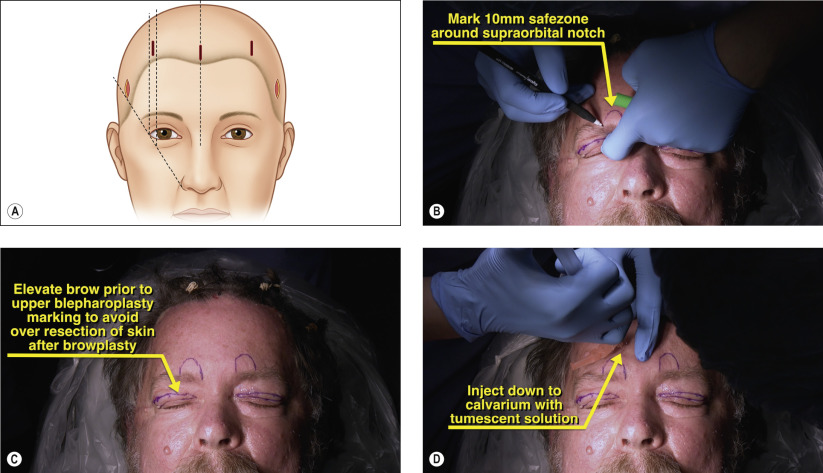
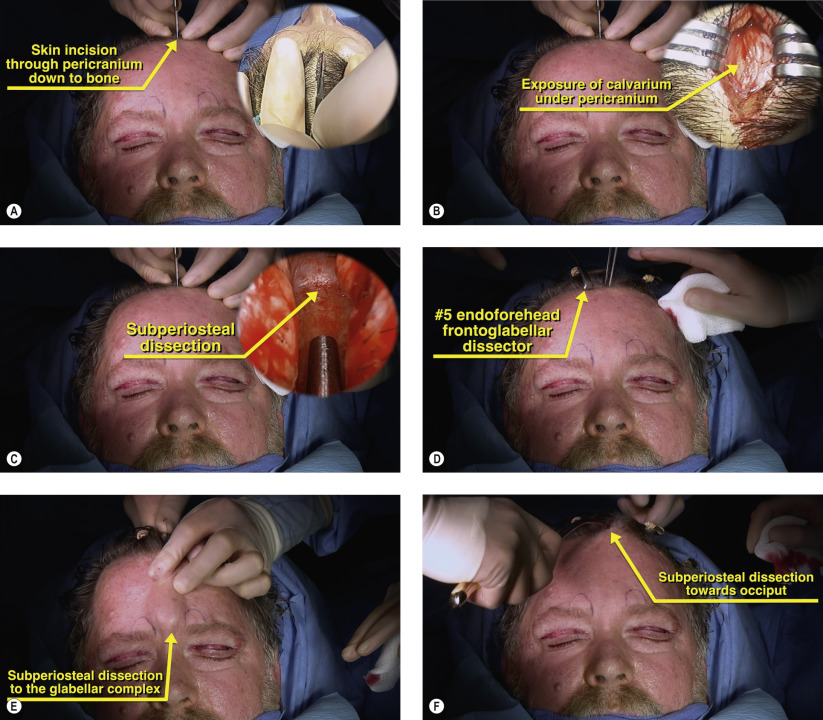
The procedure involves the creation of three optical cavities through five incisions: one central, two paramedial, and two temporal. All pockets are communicated into one larger cavity. After release of the periosteum and weakening of the brow depressors, the forehead flap is elevated and fixated. Options for central fixation include an absorbable Endotine Forehead implant (MicroAire, Charlotesville, VA) removable screw, and surgeon-drilled bone tunnels. Our preferred fixation method is use of bone tunnels. Temporally, the superficial temporalis fascia is advanced and secured to the deep temporalis fascia. Skin incisions are then closed with staples or sutures.
Surgical Technique
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


