IN THIS CHAPTER
- •
Introduction 25
- •
Patient selection 25
- •
Preoperative history and considerations 26
- •
Operative approach 26
- •
Postoperative care 30
Endoscopic abdominoplasty has very specific indications. Good to excellent skin quality combined with excess adiposity and diastasis recti is a treatable condition (signs and symptoms). This procedure consists of thorough abdominal liposuction combined with correction of muscular diastasis, performed under endoscopic control through easily concealed and usually invisible umbilical and pubic incisions.
Introduction
Endoscopic abdominoplasty is a minimally invasive procedure, usually without visible scars performed on selected patients. It is indicated for those few patients with excess abdominal adiposity and muscular diastasis, but without excessive skin laxity. Appropriate candidates represent less than 5% of patients seeking body contouring. This procedure requires endoscopic instrumentation and the ability to perform endoscopically controlled suturing at a distance. For patients that meet the criteria of excess adiposity, and muscular diastasis, without significant skin laxity, this procedure can offer pleasing results without visible scarring.
Introduction
Endoscopic abdominoplasty is a minimally invasive procedure, usually without visible scars performed on selected patients. It is indicated for those few patients with excess abdominal adiposity and muscular diastasis, but without excessive skin laxity. Appropriate candidates represent less than 5% of patients seeking body contouring. This procedure requires endoscopic instrumentation and the ability to perform endoscopically controlled suturing at a distance. For patients that meet the criteria of excess adiposity, and muscular diastasis, without significant skin laxity, this procedure can offer pleasing results without visible scarring.
Patient Selection ( Box 4.1 )
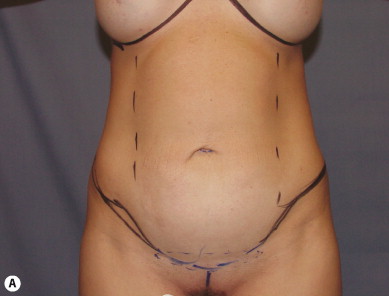
Patients who are appropriate candidates for endoscopic abdominoplasty are usually close to their ideal body weight but may have excess abdominal adiposity, muscular diastasis, and minimal skin and soft-tissue laxity ( Fig. 4.1 ). These patients represent a small number of those seeking abdominal contouring, and often present interested in liposuction unaware of the option of endoscopic abdominoplasty. Appropriate candidates should be counseled as to the availability of this procedure. Patients with excessive skin and soft-tissue laxity are not good candidates for this procedure and can experience a worsening of their condition, requiring subsequent skin resection.




The relative contraindications for all abdominal contouring procedures where the abdominal soft tissue is elevated and there is myofascial plication are similar.
Excess soft-tissue laxity that would benefit from formal resection is the most common contraindication to endoscopic abdominoplasty. These patients are better served by a mini or full abdominoplasty where excess skin and soft tissue can be resected inferiorly.
Endoscopic abdominoplasty patients are usually younger and healthier than patients undergoing full or circumferential abdominoplasty. The following is a list of relative contraindications:
- •
Smoking
- •
Diabetes mellitus
- •
Malnutrition
- •
Wound-healing disorders
- •
Bowel/bladder dysfunction
- •
Immune deficiency
- •
Medications that inhibit blood coagulation
- •
A significant history of pulmonary or deep vein thrombosis
- •
Lower extremity lymphedema/venous insufficiency
- •
Significant medical problems, including COPD/pulmonary issues, renal insufficiency, anemia, and other systemic issues that may make abdominal tightening surgery dangerous
Note: Age alone should not be a contraindication to abdominoplasty procedures if the patient is in good health. Patients who have a history of chronic pain should also be approached cautiously, as postoperative care may be significantly affected.
Preoperative History and Considerations ( Box 4.2 )
The extent of excess abdominal adiposity, skin condition and quality, including the presence and extent of striae, and the degree of muscular diastasis must all be taken into account when performing endoscopic abdominoplasty.
Most abdominal contouring procedures have similar preoperative requirements. Because the abdominal soft tissue in endoscopic abdominoplasty maintains a greater blood supply, the danger of healing problems and perfusion issues is less than with full/extended or circumferential abdominoplasty.
- •
Smoking cessation/avoidance of nicotine exposure for 4–6 weeks prior to surgery is preferred. For more extensive abdominal contouring procedures this is a strict requirement
- •
Multivitamin daily
- •
Stop aspirin/other blood thinning products with primary care doctor’s permission
- •
Abstain from all dietary/herbal supplements not approved by the surgeon
- •
Basic laboratory work should be tailored to each patient. It may include a pregnancy test, complete blood count (CBC), basic metabolic panel (BMP/Chem7), and standard coagulation profiles (PT/PTT/INR)
- •
Medical clearance if needed
- •
Wearing abdominal binder for 2 weeks before surgery
- •
Shower with a gentle antimicrobial soap the night before and day of surgery
Because these patients are usually considering only abdominal liposuction they are probably unaware of the presence of their abdominal muscle laxity or diastasis since their skin quality is reasonably good. These patients usually believe that the lower abdominal fullness is secondary to excess adiposity only, not the combination of excess adiposity and myofascial laxity. They are often also unaware of the availability of endoscopic muscle plication. When patients are told that endoscopic abdominoplasty can accomplish abdominal tightening and flattening as well as thinning, they are often interested in achieving these improved results, especially without noticeable scars.
Liposuction alone can thin the abdominal soft tissue, but without correction of rectus abdominis muscle diastasis and abdominal wall tightening, complete correction of the abdominal convexity will not be achieved. Because of this, liposuction only patients may be disappointed by surgery because of residual abdominal laxity and poor abdominal contour on lateral profile. These patients will have a thin – but not a flat – abdomen. If they have reasonably good skin quality and are close to their ideal body weight, but have excess adiposity and muscular laxity and/or diastasis recti, they are reasonable candidates for endoscopic abdominoplasty.
Surgical diagrams depicting the areas for liposuction and the incision locations for endoscopic rectus plication and suction drain placement are helpful to facilitate patient discussion and education.
Operative Approach
Preoperative markings are made as for a complete abdominal liposuction procedure. They should be made with the patient standing. The areas that will undergo liposuction, including the mons, lower abdomen, epigastric region, hip rolls, flanks and lateral breast, are marked. Surgical incisions in the periumbilical and mons areas and drain locations should also be marked. Additional inframammary liposuction incisions to address the axilla are usually not necessary. Incision placement vertically within the hair-bearing mons and within the umbilicus should be marked, as well as the lateral borders of the rectus abdominis muscle. This is the internal extent of undermining ( Fig. 4.2 , Table 4.1 ).

| Zero-degree endoscope |
| Light source, camera, monitor |
| Lighted retractor |
| Regular and extended electrocautery |
| Endoscopic needle holder |
| Insulated endoscopic electrocautery |
| Defogging agent |
| Suction (connected to endoscopic electrocautery or extended cannula) |
| Plication suture |
General, epidural, or dissociative anesthesias are all reasonable options. Muscular relaxation is desirable during this procedure to allow proper myofascial plication to be performed. Because of this requirement, general anesthesia is preferred. Sequential compression pumps are placed prior to the induction of anesthesia.
In the supine position tumescent infiltration is performed throughout all areas of subcutaneous fat to be suctioned ( Fig. 4.3 ). The normal tumescent infiltration volume is between 3 and 5 L, depending on the amount of subcutaneous fat. Sufficient time should be allowed between infiltration and liposuction to optimize the vasoconstrictive effect of the epinephrine. This will minimize blood loss during liposuction.










