Fig. 17.1
Molecular constituents of desmosomes
Keratinocytes adhere to basement membrane mainly by hemidesmosomes. The core of the hemidesmosome consists of four transmembrane proteins: BP180/type XVII collagen/BPAG2, α[alpha]6 and β[beta]4 integrins, and CD151 [7]. Both BP180 and α[alpha]6β[beta]4 integrin interact with laminin-332 at the extracellular space [8]. BP180 interacts with BP230/BPAG1e intracellularly, and α[alpha]6β[beta]4 integrin interacts with plectin in the cytoplasm [9, 10]. Both BP230 and plectin belong to the plakin family proteins, targets for paraneoplastic pemphigus [11]. Both BP230 and plectin adhere to keratin intermediate filaments [12, 13]. Molecular components of hemidesmosomes are summarized in Fig. 17.2.
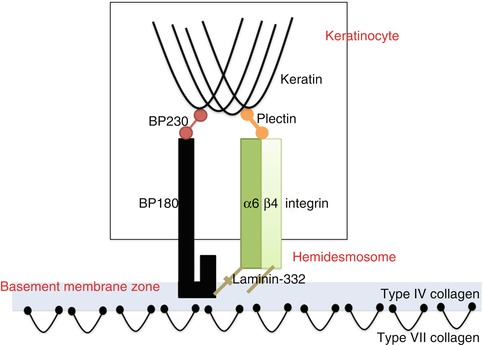
Fig. 17.2
Molecular constituents of hemidesmosomes
17.3 Autoimmune Bullous Diseases Targeting Desmosomal Proteins
Classic pemphigus is the prototype of this group. Classic pemphigus is an autoimmune bullous disease with autoantibodies against Dsgs [14]. Histopathologically, pemphigus patients show intraepidermal blister and acantholysis [15]. Classic pemphigus is divided into two major subtypes, pemphigus vulgaris and pemphigus foliaceus [14]. The autoantigen for pemphigus vulgaris is Dsg3 and that for pemphigus foliaceus is Dsg1 [14]. Pemphigus vegetans is the variant of pemphigus vulgaris, and pemphigus erythematosus is that of pemphigus foliaceus [16–19]. Other minor subtypes of pemphigus include IgA pemphigus, pemphigus herpetiformis, and paraneoplastic pemphigus [20–22].
The desmoglein compensation theory can explain the phenotypic differences among the aforementioned various subtypes of pemphigus [23]. The amount and distribution of Dsg1 and Dsg3 are different in the skin and the oral mucosa (Fig. 17.3). In the skin, the expression of Dsg1 is found throughout the entire epidermis but particularly strong in the upper epidermis. On the other hand, the expression of Dsg3 is limited to the basal and suprabasal epidermis. In contrast, in the oral mucosa, both Dsg1 and Dsg3 are found throughout the entire epithelium, but the Dsg1 expression is much weaker than Dsg3. Therefore, in mucosal-dominant-type pemphigus vulgaris with anti-Dsg3 antibodies, oral mucosal lesion occurs because the remaining Dsg1 cannot compensate for mucosal epithelial cell-cell adhesion. In contrast, skin lesions are mild, because the remaining Dsg1 can compensate for the epidermal cell-cell adhesion. In pemphigus foliaceus with anti-Dsg1 antibodies, oral mucosal lesions are not seen, because quantitatively a large amount of Dsg3 in the oral mucosa can compensate for the loss of Dsg1. In contrast, skin lesions occur, because the remaining Dsg3 cannot compensate for the cell-cell adhesion in the upper epidermis. In mucocutaneous-type pemphigus vulgaris with antibodies to both Dsg3 and Dsg1, no cell-cell adhesion remains.
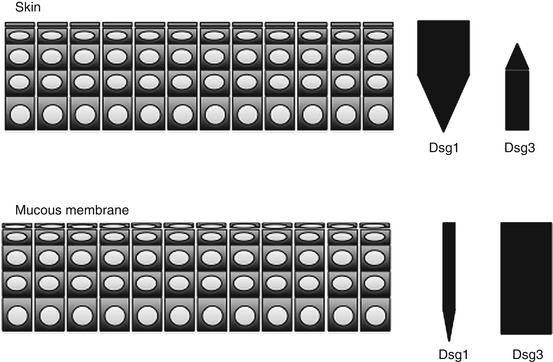
Fig. 17.3
Expression of desmogleins in the skin and mucous membrane
17.4 Autoimmune Diseases Targeting Keratinocyte-Extracellular Matrix Adhesion
The prototype of this disease group is bullous pemphigoid. Bullous pemphigoid is the most common autoimmune bullous disease [24, 25]. Bullous pemphigoid is characterized clinically by tense blisters and erythema, caused by IgG autoantibodies to BP180 and BP230 [26]. Bullous pemphigoid is considered to be developed by the following pathomechanism. Binding of IgG anti-BP180 autoantibodies to BP180 causes neutrophilic and eosinophilic migration and secretion of proteolytic enzymes, which results in proteolysis of component proteins in basement membrane zone [27–29]. In addition, endocytosis of BP180 after the binding with autoantibodies is also suggested to play a role in the pathogenesis [30, 31]. Some studies suggested that anti-BP230 antibodies are also pathogenic in bullous pemphigoid [32, 33].
Other diseases categorized as autoimmune subepidermal bullous diseases are mucous membrane pemphigoid, anti-laminin γ[gamma]1 pemphigoid (formerly, anti-p200 pemphigoid), herpes gestationis, herpetiform dermatosis (Duhring), linear IgA bullous dermatosis, and epidermolysis bullosa acquisita [34–38].
17.5 Enzyme-Linked Immunosorbent Assay (ELISA), Basics
ELISA is a plate-based immunoassay which is used to detect autoantibodies in various autoimmune diseases, including autoimmune bullous diseases. In ELISA, recombinant proteins of target autoantigens are immobilized to a solid surface of the plates, which are then incubated with autoantibodies in the patient sera, followed by incubation with second antibody conjugated with horseradish peroxidase [39]. Detection is achieved by enzyme activity of these peroxidases via incubation with chromogen [39]. The principle of ELISA for the detection of pemphigus autoantibodies is shown in Fig. 17.4.
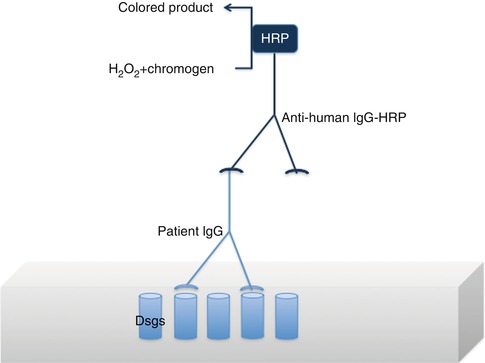
Fig. 17.4
Principle of ELISA
17.6 Application of ELISA to Diagnose Autoimmune Bullous Diseases
ELISA assay alone is insufficient to diagnose AIBD; the patient has to have typical clinical features, histopathology and positive direct IF, because unaffected patients can have non-pathogenic antibodies in the sera. ELISA assay is currently available for several autoimmune bullous diseases, including pemphigus vulgaris, pemphigus foliaceus, bullous pemphigoid, and epidermolysis bullosa acquisita, to both make diagnosis and monitor the clinical course in these diseases. Historically, ELISAs are first developed for the diagnosis of pemphigus vulgaris and pemphigus foliaceus in 1997 [40]. The recombinant proteins of full length of extracellular domains of Dsg3 and Dsg1 were produced by baculovirus expression system [40]. The first ELISA for bullous pemphigoid using recombinant protein of BP180 NC16a domain produced by E. coli expression was developed in 2002 [41]. The ELISA using recombinant proteins of N- and C-terminal domains of BP230 produced by E. coli expression was also developed [42].
Using ELISAs of both Dsg1 and Dsg3, serological diagnosis of mucosal-dominant-type pemphigus vulgaris, mucocutaneous-type pemphigus vulgaris, and pemphigus foliaceus became possible [43]. Positive Dsg3 ELISA with negative Dsg1 ELISA means mucosal-dominant-type pemphigus vulgaris. Positive Dsg1 ELISA with negative Dsg3 ELISA means pemphigus foliaceus. Double positive by ELISAs for both Dsg1 and Dsg3 means mucocutaneous-type pemphigus vulgaris. However, clinical and histopathological findings are also required to diagnose correctly these diseases. The specificity and sensitivity of Dsg3 ELISA for a diagnosis of pemphigus are 94 and 96 %, respectively, and those of Dsg1 ELISA are 96 and 96 % [40].
ELISA of both BP180 and BP230 with concomitant use of histopathology and direct immunofluorescence study can confirm the diagnosis of pemphigoid. The specificity and sensitivity of BP180 ELISA for a diagnosis of bullous pemphigoid are 84.4 and 98.9 %, respectively, and those of BP230 ELISA are 72.4 and 99.5 % [41, 42].
ELISAs of Dsgs and BP180/BP230 are useful for monitoring disease activity for pemphigus and pemphigoid, respectively [41, 42]. The effect of steroids and determination of steroid dose can be assessed by monitoring ELISA indices [44]. Moreover, clearance of autoantibodies before and after plasmapheresis can also be confirmed [45].
An ELISA for type VII collagen was recently developed for the diagnosis and disease monitoring in epidermolysis bullosa acquisita [46].
17.7 Immunoblotting, Basics
Immunoblotting is used to identify autoantigens in various autoimmune bullous diseases. Proteins are separated by electrophoresis and then transferred onto nitrocellulose or polyvinylidene difluoride membrane [47]. The membrane is overlaid with patient sera and then with second antibodies to human IgG or IgA conjugated with horseradish peroxidase or other enzymes [48, 49]. The rationale of immunoblotting is summarized in Fig. 17.5.
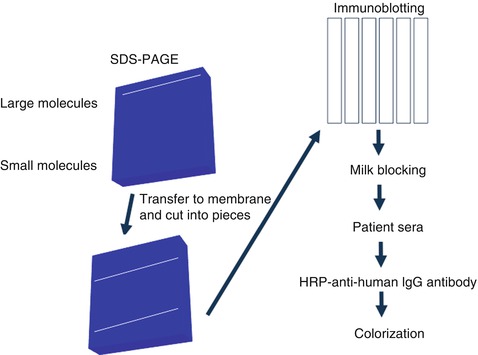
Fig. 17.5
Principle of immunoblotting
17.8 Application of Immunoblotting to Diagnose Autoimmune Bullous Diseases
Immunoblotting is a relatively easy method to be performed in any clinical laboratories. The disadvantage of immunoblotting is low sensitivity due to degeneration of target proteins during electrophoresis procedure. Currently, dermatology laboratories in Kurume University are performing a number of immunoblotting studies for different autoimmune bullous diseases, using various substrates, including normal human epidermal and dermal extracts, recombinant proteins of NC16a and C-terminal domains of BP180, purified human laminin-332, and concentrated HaCaT cell culture supernatant.
Using various combinations of these immunoblotting methods, most of the autoimmune bullous diseases can be diagnosed. By immunoblotting using normal human epidermal extract, patient IgG antibodies react with the 130 kDa Dsg3 in pemphigus vulgaris and pemphigus vegetans [50]; with the 160 kDa Dsg1 in pemphigus foliaceus, pemphigus erythematosus, and mucocutaneous-type pemphigus vulgaris [51]; with the 210 kDa envoplakin and the 190 kDa periplakin in paraneoplastic pemphigus [52]; with the 180 kDa BP180 in bullous pemphigoid, mucous membrane pemphigoid, and herpes gestationis [50, 53, 54]; and with the 230 kDa BP230 in bullous pemphigoid [50]. Moreover, IgG antibodies in various diseases react with different antigens by immunoblotting, i.e., bullous pemphigoid reacts with recombinant protein of BP180 NC16a domain [55], anti-BP180-type mucous membrane pemphigoid reacts with recombinant protein of BP180 C-terminal domain [56], and anti-laminin-332-type mucous membrane pemphigoid reacts with purified human laminin-332 [57]. By IgG immunoblotting using normal human dermal extract, epidermolysis bullosa acquisita reacts with the 290-kDa-type VII collagen [50], and anti-laminin-γ[gamma]1 pemphigoid reacts with the 200 kDa laminin-γ[gamma]1 [35]. In lamina lucida-type linear IgA bullous dermatosis, patient IgA antibodies react with the 97 kDa LAD-1 in normal human epidermal extract [58]. In addition, by immunoblotting using concentrated HaCaT cell culture supernatants, patient IgA antibodies react with the 120-Da LAD-1 [59]. In sublamina densa-type linear IgA bullous dermatosis, by immunoblotting using normal human dermal extract, patient IgA antibodies rarely react with type VII collagen [60], but the autoantigens for most of these patients are still unknown. Representative immunoblotting results for mucocutaneous-type pemphigus vulgaris, paraneoplastic pemphigus, bullous pemphigoid, anti-BP180-type mucous membrane pemphigoid, and epidermolysis bullosa acquisita and anti-laminin-γ[gamma]1 pemphigoid and anti-laminin-332-type mucous membrane pemphigoid are shown in Fig. 17.6.
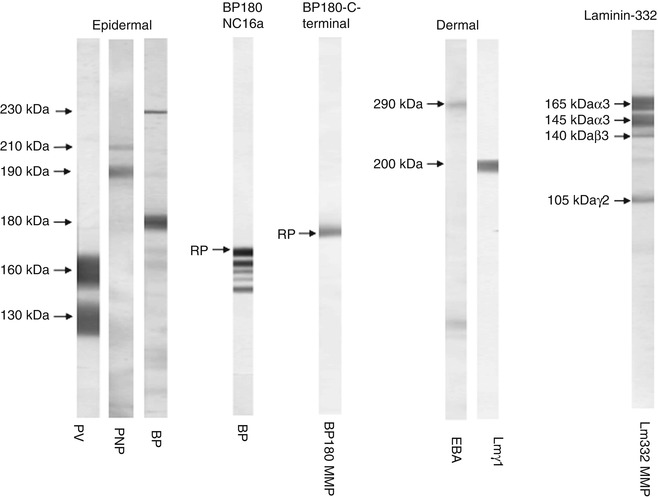
Fig. 17.6
Serological diagnoses by immunoblotting using different substrates for mucocutaneous-type pemphigus vulgaris (PV), paraneoplastic pemphigus (PNP), bullous pemphigoid (BP), anti-BP180-type mucous membrane pemphigoid (BP180 MMP), and epidermolysis bullosa acquisita (EBA) and anti-laminin-γ[gamma]1 pemphigoid (Lmγ1) and anti-laminin-332-type mucous membrane pemphgoid (Lm332 MMP)
17.9 Conclusion
The combination of ELISA and immunoblotting is a powerful tool to diagnose various autoimmune bullous diseases.
References
1.
2.
3.
4.
Brooke MA, Nitoiu D, Kelsell DP. Cell-cell connectivity: desmosomes and disease. J Pathol. 2012;226(2):158–71.CrossRefPubMed
Related posts:
 Kindlin-1 and Its Role in Kindler Syndrome
Kindlin-1 and Its Role in Kindler Syndrome
 Cyclophosphamide in Autoimmune Blistering Diseases: Safety, Efficacy and Evidence Base
Management of Bullous Systemic Lupus Erythematosus
Cyclophosphamide in Autoimmune Blistering Diseases: Safety, Efficacy and Evidence Base
Management of Bullous Systemic Lupus Erythematosus
 Using Intravenous Immunoglobulins in Autoimmune Bullous Diseases
Using Intravenous Immunoglobulins in Autoimmune Bullous Diseases
 Living with Epidermolysis Bullosa: Reviewing the Impact on Individuals’ Quality of Life
Living with Epidermolysis Bullosa: Reviewing the Impact on Individuals’ Quality of Life
 How to Take a Skin Biopsy Correctly to Diagnose Epidermolysis Bullosa and Autoimmune Bullous Diseases
How to Take a Skin Biopsy Correctly to Diagnose Epidermolysis Bullosa and Autoimmune Bullous Diseases
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


