| Symptomatic cicatricial ectropion (tearing, mucoid discharge, conjunctival keratinization, corneal exposure) |
| History of trauma (chemical/burns), prior cosmetic surgery, reconstructive surgery to face (trauma/post cancer removal), actinic/radiation exposure |
| Underlying dermatologic disorders (ichthyosis, contact dermatitis, scleroderma) |
| Degree of anterior lamellar shortening |
| Presence of lower eyelid laxity, lagophthalmos, lower eyelid retraction |
| Slit lamp examination |
Introduction
Cicatricial ectropion is characterized by a deficiency in the anterior lamellae of the eyelid. This condition may occur on the upper and/or lower eyelids. With a shortage of the skin, the eyelid everts, resulting in ectropion. Functionally, this can result in tearing from poor lacrimal outflow, corneal exposure, and keratinization of the palpebral conjunctiva.
A careful history to elucidate the cause of the cicatricial ectropion is necessary to prevent recurrence after treatment. Chemical burns or thermal injury are particularly challenging to treat and often require repeated skin grafting. Chronic dermatologic conditions should be maximized medically before considering surgical treatment. Periocular reconstruction after skin cancer removal may also result in cicatricial ectropion if excessive tension is present in the vertical meridians. Blepharoplasty with excessive skin removal can result in cicatricial ectropion as well as eyelid retraction particularly when eyelid laxity is not concurrently treated.
Lysis of the anterior lamellar cicatrix followed by placement of a full thickness skin graft is the mainstay of treatment for cicatricial ectropion. Lower eyelid tightening with a subperiosteal midface lift and posterior lamellar spacer graft is useful for eyelid retraction alone, but with severe cicatricial ectropion, a skin graft is often necessary. For patients who are not candidates for skin grafting, a Z-plasty with the central limb oriented vertically can be used to treat lower eyelid cicatricial ectropion.
The decision between a full thickness or split thickness skin graft as well as donor site choices are discussed in Chapter 1 . The primary benefits of a full thickness skin graft are minimal contraction, improved color and texture, and no need for a dermatome. Multiple donor sites are available such as upper eyelid, preauricular, retroauricular, and supraclavicular ( Figure 1.22 , Figure 1.23 , Figure 1.24 , Figure 1.25 , Figure 1.26 , Figure 1.27 , Chapter 1 ). When possible the upper eyelid should be used for the most ideal match.
Postoperative management of a full thickness skin graft is equally as important as the surgery itself. Full thickness skin grafts exchange nutrients and metabolic wastes through diffusion by a process known as plasma imbibition. Within the first 24 to 48 hours, vascular inosculation between the graft and recipient bed occurs. Between 48 and 72 hours, capillary buds start to grow into the graft and, by 5 days, a blood supply has been established. Several conditions can adversely affect this process. Shearing of the graft can cause bleeding and disrupt neovascularization. A hematoma between the graft and bed affects diffusion and firm immobilization of the graft with a pressure patch is essential to maximize graft survival. Antibiotic prophylaxis can minimize infection at the interface and strict avoidance of smoking to prevent ischemia is essential.
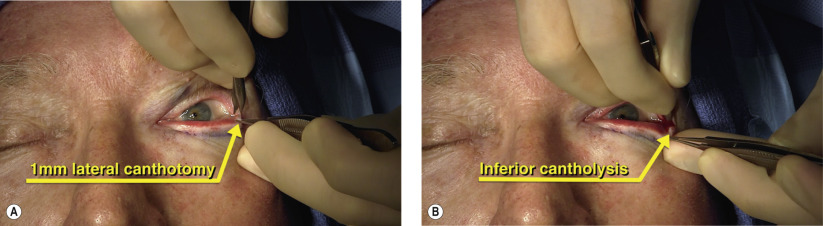
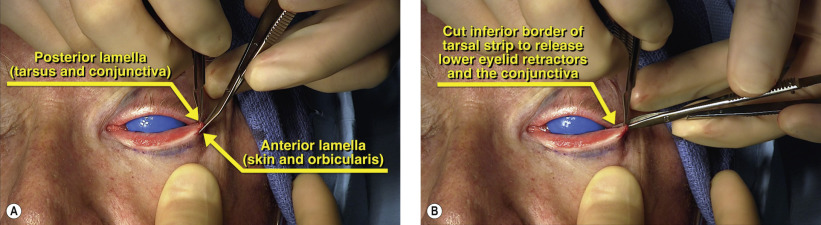
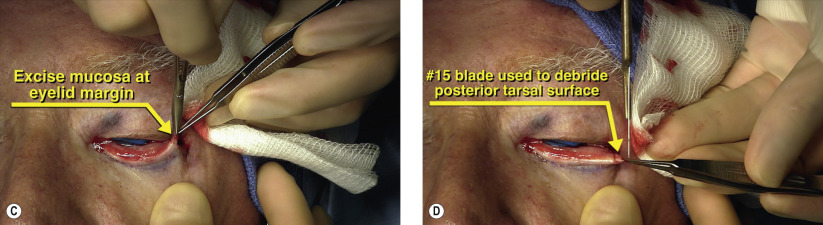
Surgical Technique
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


