Discoloration
Dermatologic findings
Etiology
Distribution
Treatment
White
Uremic frosting (rare)
Deposition of urea crystals from sweat on skin
Head and neck
Dialysis
Yellow
Pallor
Anemia, deposition of carotenoids, urochrome
Generalized
Treatment of underlying anemia of chronic disease
Evolving red/purple/green
Ecchymoses
Abnormal hemostasis
Sites of traumatic injury
Normalizing hemostasis
Brown
Hyperpigmentation
Increased circulating β-melanocyte stimulating hormone
Photo-distributed
None, resolves with renal transplantation
Xerosis and acquired ichthyosis are common problems that can be associated with hyperpigmentation in the setting of kidney disease. In darker skinned patients there may be a greyish or “ashy” appearance to the dry skin. Many patients experience pruritus secondary to the xerosis and uremia which ultimately leads to mechanical manipulation of skin and associated secondary hyperpigmentation and sometimes lichenification. Symptomatic treatment includes liberal use of emollients to moisturize the skin. Topical antipruritics such as menthol containing lotions provide temporary relief due to a cooling effect when applied to the skin. If pruritus is associated with an underlying severe hyperparathyroidism, parathyroidectomy may be indicated [5]. Narrowband ultraviolet B (NB-UVB) phototherapy may be effective in relieving uremic pruritus but does not alter the associated dyspigmentation and may, in fact, induce further hyperpigmentation due to the tanning response.
Diseases That Affect the Kidney and Skin with Associated Dyschromia
Connective tissue diseases (e.g., systemic lupus erythematosus (SLE), systemic sclerosis) are systemic diseases with significant dermatologic and nephrologic effects. Specific dermatologic findings of these conditions are found in other chapters of this book. They are included here for a complete discussion of dyschromias.
SLE is a systemic connective tissue disease with a wide array of symptoms and signs. Cutaneous involvement is significant and 4 of the 11 diagnostic criteria of SLE are mucocutaneous findings (Table 8.2). Several eruptions of SLE have archetypal descriptions in which dyspigmentation is a prominent finding. The malar rash, classically described as the “butterfly rash,” consists of facial erythema across malar cheeks and bridge of the nose. In comparison, discoid lupus typically demonstrates areas of hyperpigmentation and depigmentation especially in darker skinned patients. Other cutaneous manifestations of SLE include periungual telangiectasia, oral mucosal hemorrhages, and a livedoid reaction pattern, most commonly found on the lower legs.
Table 8.2
American College of Rheumatology: SLE diagnostic criteria
Malar rash |
Discoid rash |
Photosensitivity |
Oral ulceration |
Arthritis |
Proteinuria >0.5 g/day or casts |
Neurologic disorders |
Serositis |
Hematologic abnormalities |
Immunologic disorders |
ANA positivity |
Multidisciplinary treatment approaches are best. From a dermatologic standpoint photoprotection is of utmost importance. Sun avoidance is optimal; however, daily use of a high sun protection factor sunblock should be recommended to those who cannot completely avoid the sun [2]. Skin directed therapy includes the use of potent topical steroids, with topical calcineurin inhibitors being second line topical therapy. First line systemic treatment involves the use of antimalarial drugs; hydroxychloroquine is most commonly used. Ocular toxicity is rare but baseline and follow-up retinal examinations are required to monitor for retinal toxicity; the risk of retinal toxicity may increase with cumulative dose. A more common side effect of hydroxychloroquine is an idiosyncratic development of hyperpigmentation. Other more aggressive treatment options for cutaneous lupus are beyond the scope of this chapter.
Systemic sclerosis, an autoimmune connective tissue disease characterized by anti-Scl-70, anticentromere and antinuclear antibodies, can ultimately lead to progressive sclerosis of the skin and internal organs with significant involvement of the kidney. Established cutaneous disease demonstrates a classic “salt and pepper” mottled dyspigmentation on the trunk and scalp. Raynaud phenomenon is common in systemic sclerosis causing prominent dyspigmentation including pallor, cyanosis, and reactive hyperemia.
Treatment with angiotensin inhibitors and angiotensin II receptor antagonists has improved renal morbidity significantly [6]. Skin directed therapies remain unsatisfactory with limited efficacy (Fig. 8.1).

Fig. 8.1
Salt and pepper dyspigmentation in scleroderma. Image reprinted with permission from Jeffrey P. Callen, M.D. University of Louisville School of Medicine, published by Medscape Reference (http://emedicine.medscape.com/), 2014, available at: http://emedicine.medscape.com/article/1049648-overview
Genodermatoses are inherited disorders that have characteristic skin findings; a subset of these conditions affects the kidney and is associated with pigmentary alteration.
Fabry disease, an X-linked lysosomal storage disorder leads to accumulation of neutral glycosphingolipids in multiple organ systems including the kidney. It is caused by mutations in the α-galactosidase A gene. Patients present with characteristic skin findings of multiple reddish-brown papules in a classic bathing suit distribution. Macular angiomas may also be seen on the proximal extremities, palmar and plantar surfaces, periungually and on the vermillion border of the lips. Cutaneous vascular lesions can be treated with intense pulse light (IPL) and other vascular lasers to improve cosmesis [7].
Familial Mediterranean fever is an inherited disorder due to mutations in the MEFV gene which encodes a pyrin protein important in the inflammatory pathway. The hallmark findings of the disorder are recurrent episodes of serositis, involving the lungs, heart, peritoneum, and joints, with an associated periodic fever. In a subset of patients recurrent inflammation results in excess production of amyloid A protein with aberrant deposition in the kidneys leading to eventual renal insufficiency. Patients often present with a “hot ankle rash,” consisting of erythematous, erysipelas-like patches on bilateral lower legs. Treatment with colchicine may suppresses attacks and prevent associated amyloid deposition in tissues; anti-interleukin (IL)-1 biologics may be successful in colchicine-resistent cases.
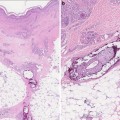
Primary systemic amyloidosis is the most common type of systemic amyloidosis and is usually associated with a plasma cell dyscrasia. There is deposition of light chain amyloid in internal organs including the kidneys which can lead to chronic renal failure; Bence Jones proteins are usually detected in the urine. Cutaneous lesions due to amyloid deposits are rarely seen in primary systemic amyloidosis; however, when present, the most characteristic, and likely pathognomonic, color change is the development of bilateral purpura of the eyelids called “pinch purpura”. Similar purpuric lesions and may also be present on the upper trunk, face, and neck. Other less frequent findings are translucent flesh-colored papules on the face, neck, and scalp. Smooth, waxy, infiltrated papules, and plaques may be evident on the palms and fingertips. Skin biopsy may be necessary to make a diagnosis.
Nephrogenic systemic fibrosis is a rare and relatively recently described skin disorder [8]. While the exact etiology is yet to be elucidated, it is associated with exposure to gadolinium based contrast agents used in magnetic resonance imaging in patients with renal insufficiency [8]. Initial cutaneous changes are symmetrical red or deeper colored papules and plaques on the lower extremities with progressive swelling and tightening of the skin. Later stage disease has an indurated peau d’orange appearance of the extremities often with associated hyperpigmentation. Fibrosis may also involve extracutaneous sites including the heart, lungs, and the skeletal muscle and the sclera which can have yellowish plaques. There is no known effective treatment. Therapy is usually directed at optimizing renal function. Other therapies, with limited success include phototherapy, extracorporeal photophoresis, sodium thiosulfate, and rapamycin. Physical therapy is an adjunctive modality highly recommended to maintain functional mobility in affected patients [2, 8, 9].
Vasculitides
This group of disorders is traditionally classified according to the size of the affected vessels. Vasculitides are well known to have associated underlying kidney diseases and prominent characteristic cutaneous findings. There are several major vasculitides that are commonly associated with renal disease and which can have dyspigmentation as a prominent dermatologic sign. The following are discussed in this section.




1.
Leukocytoclastic vasculitis
2.
Henoch–Schönlein purpura
3.
Polyarteritis nodosa
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
