Dupuytren’s Disease
Ghazi M. Rayan
Dupuytren disease (DD) is a fibroproliferative disorder that afflicts primarily the hands with the development of pathologic tissue that originates from existing normal palmar fascial structures. The etiology is unknown, the pathology is diverse, and diagnosis can be difficult in the early stages. The treatment can be challenging, and there is potential for recurrence. The prognosis is variable depending on the patient’s diathesis or degree of genetic predisposition.
I. Fascial Anatomy
The palmar fascial complex (Fig. 24.1) of the hand has five components: the radial, ulnar, and central aponeuroses, the palmodigital fascia, and the digital fascia.
The radial aponeurosis has four components:
The thenar fascia
The thumb pretendinous band
The distal commissural ligament
The proximal commissural ligament
The ulnar aponeurosis consists of three components:
The hypothenar muscle fascia
The pretendinous band to the small finger
The abductor digiti minimi soft tissue coalescence
The central aponeurosis is a triangular fascial layer. The apex is located at the proximal aspect and the fibers extend distally and are oriented longitudinally, transversely, and vertically.
The longitudinal fibers fan out as pretendinous bands of the three central digits.
The transverse fibers make up the natatory ligament located in the distal part of the palm and the transverse ligament of the palmar aponeurosis (TLPA), which is located proximally and gives origin to the septa of Legueu and Juvara. The TLPA distal radial extent is the proximal commissural ligament.
The vertical fibers of the central aponeurosis are the minute vertical bands of Grapow and the septa of Legueu and Juvara. The vertical bands are numerous, small, strong, and scattered along the palmar fascial complex, and are most abundant in the central aponeurosis. There are eight vertical septa of Legueu and Juvara (one along the radial aspect and one along the ulnar aspect of each finger) (Fig. 24.2), forming seven compartments: four flexor septal canals that contain the flexor tendons and three web space canals that contain the common digital nerves and arteries and the lumbrical muscles.
The palmodigital fascia is a confluence of several retinacular structures located between the palm and digits, the most important of which is the spiral band that connects the palmar and digital fascial structures.
The digital fascia components surround the neurovascular structures, and consist of Grayson ligament volar, Cleland ligament volar, and the lateral digital sheet of Gossett.
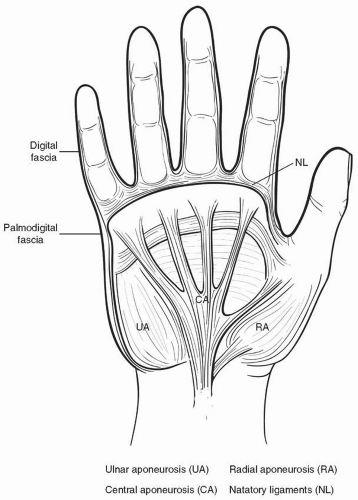 Figure 24.1 An illustration of the five components of the palmar fascial complex. |
II. Pathology
Dupuytren nodules and cords are pathognomonic of DD. In DD, normal fascial bands become diseased cords. Typically, these cords progressively shorten, leading to joint and soft-tissue contractures. These shortened cords cause joint deformity, and the long-standing flexion deformity leads to contracture of the capsuloligamentous tissue and attenuation of the dorsal gliding structures causing flexion contractures of the
metacarpophalangeal and proximal interphalangeal joints. There are many pathologic structures encountered in DD.
metacarpophalangeal and proximal interphalangeal joints. There are many pathologic structures encountered in DD.
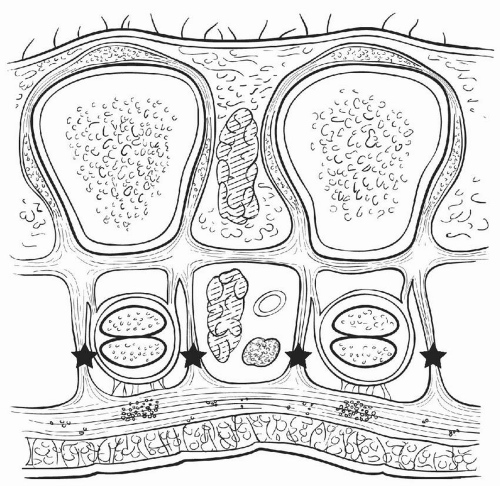 Figure 24.2 An illustration of the septa of Legueu and Juvara*. |
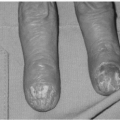
Microcords are the diseased Grapow vertical bands. They lead to skin thickening, which is one of the earliest manifestations of DD. These can mimic callus formation and make diagnosing early disease difficult.
Skin pits are small-depressions in the palmar skin surface. They are pathognomonic of DD and develop from the superficial fibers of the pretendinous band that became diseased, pulling on their attachments into the dermis.
The pretendinous cord develops from the pretendinous band and is the cord most frequently seen in DD. It is responsible for flexion deformity of the metacarpophalangeal joint.
The vertical cord is the diseased septa of Legueu and Juvara, which is located between the flexor tendon sheath and neurovascular bundles. Its presence may be responsible for the associated stenosing tenosynovitis that is encountered with DD.
The spiral cord has four origins:
The pretendinous band
The spiral band
The lateral digital sheet
Grayson ligament
This cord is encountered most often in the small finger. Initially, the cord spirals around the neurovascular bundle, but as it contracts, the cord straightens and the neurovascular bundle spirals around the cord, displacing proximally, superficially, and toward the middle of the digit. This distorted anatomy of the neurovascular bundle renders it at risk during surgery.
The natatory cord develops from the natatory ligament, converting the u-shaped web-space fibers into a v shape and producing contracture of the second, third, and fourth web spaces.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree