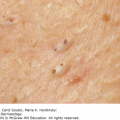
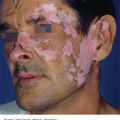
25 Almost any drug can cause a cutaneous reaction, and many inflammatory skin conditions can be caused or exacerbated by drugs. A drug reaction can reasonably be included in the differential diagnosis of most skin diseases. These are many and various (Table 25.1), being related both to the properties of the drug in question and to a variety of host factors. Drug trials have traditionally studied average population responses to drugs, but the increasing ease with which genetic differences between individuals can be measured offers the promise of personalized medicine. Genetically predicted variations in response – both beneficial and adverse – to a drug will be used to guide the right dose and type of drug for individual patients (pharmacogenetics). For example, drug-induced lupus erythematosus occurs more commonly among ‘slow acetylators’ who take hydralazine. However, not all adverse drug reactions have a genetic basis; the excess of drug eruptions seen in the elderly may reflect drug interactions associated with their high medication intake. Table 25.1 Some mechanisms involved in drug reactions. Not all drug reactions are based on allergy. Some are a result of overdosage, others to the accumulation of drugs or to unwanted pharmacological effects (e.g. stretch marks from systemic steroids; Figure 25.1). Other reactions are idiosyncratic (an odd reaction peculiar to one individual) or a result of alterations of ecological balance (see below). Figure 25.1 Gross striae caused by systemic steroids. Cutaneous reactions can be expected from the very nature of some drugs. These are normal but unwanted responses. Patients show them when a drug is given in a high dose, or even in a therapeutic dose. For example, mouth ulcers may occur as a result of the cytotoxicity of methotrexate. Silver-based preparations, given for prolonged periods, can lead to a slate-grey colour of the skin (argyria). Acute vaginal candidiasis occurs when antibiotics remove the normal resident bacteria from the female genital tract and so foster colonization by yeasts. Dapsone or rifampicin, given to patients with lepromatous leprosy, may cause erythema nodosum leprosum as the immune response to the bacillus is re-established. Non-allergic reactions are often predictable. They affect many, or even all, patients taking the drug at a sufficient dosage for a sufficient time. Careful studies before marketing should indicate the types of reaction that can be anticipated. Allergic drug reactions are less predictable. They occur in only a minority of patients receiving a drug and can do so even with low doses. Allergic reactions are not a normal biological effect of the drug and usually appear after the latent period required for induction of an immune response. Chemically related drugs may cross-react. The majority of allergic drug reactions are caused by type IV cell-mediated immune reactions (p. 25), which can present in a number of forms, most commonly a maculopapular eruption or morbilliform erythema. Rarer allergic reactions include bullae, erythroderma, pruritus, toxic epidermal necrolysis (TEN), acute generalized exanthematous pustulosis (AGEP) and the drug rash with eosinophilia and systemic signs (DRESS) syndrome. Helper CD4+ T cells occur more frequently in the more common morbilliform eruptions, while cytotoxic CD8+ T cells predominate in blistering eruptions (TEN, Stevens–Johnson syndrome) and fixed drug eruptions. Other types of drug reaction include urticaria and angioedema, generally resulting from IgE-mediated type I hypersensitivity reactions, and vasculitis generally caused by type III immune complex-mediated reactions (p. 25). The factors that lead to particular clinical patterns of cutaneous adverse drug reactions remain largely unexplained. Experience helps here, together with a knowledge of the reactions most likely to be caused by individual drugs, and also of the most common causes of the various reaction patterns. Any unusual rash, especially if polymorphic (variation in appearance of rash), should be suspected of being a drug reaction, and approached along the lines listed in Table 25.2. Table 25.2 The six vital questions to be asked when a drug eruption is suspected. Penicillins and sulfonamides are among the drugs most commonly causing allergic reactions. These are often morbilliform (Figure 25.2), but urticaria, erythema multiforme and fixed eruptions are common too. Viral infections are often associated with exanthems, and many rashes are incorrectly blamed on an antibiotic when, in fact, the virus was responsible. Most patients with infectious mononucleosis develop a morbilliform rash if ampicillin is administered. Penicillin is a common cause of severe anaphylactic reactions, which can be life-threatening. Minocycline can accumulate in the tissues and produce a brown or grey colour in the mucosa, sun-exposed areas or at sites of inflammation, as in the lesions of acne. Minocycline can rarely cause the hypersensitivity syndrome reaction, hepatitis, worsen lupus erythematosus or elicit a transient lupus-like syndrome. Trimethoprim, now regularly used as a second-line antibiotic for the treatment of acne, can cause an idiosyncratic eruption between days 7 and 14 of therapy; the rash is usually maculopapular or morbilliform in appearance but TEN has been reported. Figure 25.2 Symmetrical erythematous maculopapular rash as a result of ampicillin. Like penicillin itself, penicillamine can cause morbilliform eruptions or urticaria, but the drug has also been incriminated as a cause of haemorrhagic bullae at sites of trauma, of the extrusion of elastic tissue through the skin, and of pemphigus. Reactions to these are less common now that their hormonal content is small. The hair fall that may follow stopping the drug is like that seen after pregnancy (telogen effluvium; p. 178). Chloasma, hirsutism, erythema nodosum, acne and photosensitivity may also occur. This frequently causes rashes. Its side effects range from pruritus to morbilliform eruptions, to curious papulosquamous eruptions such as pityriasis rosea or lichen planus. Erythroderma, erythema nodosum, hair fall and stomatitis may also be provoked by gold. Cutaneous side effects from systemic steroids include a ruddy face, cutaneous atrophy, striae (Figure 25.1), hirsutism, an acneiform eruption and a susceptibility to cutaneous infections, which may be atypical. Skin reactions to phenytoin, carbamazepine, lamotrigine and phenobarbitol are common and include erythematous, morbilliform, urticarial and purpuric rashes. TEN, erythema multiforme, exfoliative dermatitis, DRESS and a lupus erythematosus-like syndrome are fortunately rarer. About 1% of patients taking lamotrigine develop Stevens–Johnson syndrome or TEN. A phenytoin-induced pseudolymphoma syndrome has also been described in which fever and arthralgia are accompanied by generalized lymphadenopathy and hepatosplenomegaly and, sometimes, some of the above skin signs. Long-term treatment with phenytoin may cause gingival hyperplasia (Figure 25.3) and coarsening of the features as a result of fibroblast proliferation. Figure 25.3 Gingival hyperplasia caused by long-term phenytoin treatment.
Drug Eruptions
Mechanisms
Pharmacological
Caused by overdosage or failure to excrete or metabolize
Cumulative effects
Altered skin ecology
Allergic
IgE-mediated
Cytotoxic
Immune complex-mediated
Cell-mediated
Idiosyncratic
Exacerbation of pre-existing skin conditions
Non-allergic drug reactions

Allergic drug reactions
Presentation
Some drugs and the reactions they can cause
Antibiotics

Penicillamine
Oral contraceptives
Gold
Steroids
Anticonvulsants

Highly active antiretroviral drugs
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


