Direct-to-Implant Breast Reconstruction
Amy S. Colwell
Eric J. Wright
DEFINITION
Following mastectomy, the reconstructive goal is to recreate a natural-appearing breast, which may improve quality of life and body image.
Direct-to-implant (DTI) reconstruction involves placement of the permanent implant at the time of mastectomy in one stage.
DTI reconstruction is a cost-effective, low complication rate procedure with outcomes similar to two-stage tissue expander/implant reconstruction in experienced centers.1
Alternatives to DTI include no reconstruction, two-stage tissue expander/implant reconstruction and autologous reconstruction with flaps or fat.
In comparison with tissue expander reconstruction, there are fewer office visits and one less surgical procedure. Compared to autologous reconstruction, there is no donor site morbidity.
ANATOMY
The breast skin is preserved or reduced to accommodate an appropriate-size implant.
Skin-sparing or nipple-sparing mastectomy keeps the native breast skin envelope intact by crafting a natural shape with immediate round or shaped implant insertion. In nipplesparing procedures, the nipple ducts are removed with the mastectomy and the outer epidermis and dermis are retained with the rest of the breast skin.
Ideal candidates for nipple-sparing mastectomy have grade 1 to grade 2 nipple ptosis.
Patients with grade 3 ptosis may be better candidates for skin-sparing mastectomy or mastopexy prior to mastectomy.
The implant has total, partial, or no muscle coverage under the breast skin.
The pectoralis major muscle most commonly covers the implant superiorly. Inferiorly, acellular dermal matrix (ADM) or mesh serves as an extension of the pectoralis major muscle to cover the implant inferiorly.
PATIENT HISTORY AND PHYSICAL FINDINGS
DTI reconstruction can be performed in unilateral or bilateral mastectomies and in reconstruction for cancer or prophylaxis.
Ideal candidates for DTI reconstruction are otherwise healthy patients, with moderate size breasts, who desire to retain approximately the same breast size.
Patients who desire a significantly larger size are more safely treated with tissue expander/implant reconstruction.
Relative contraindications to DTI include active smoking, uncontrolled diabetes, and immunosuppressive medications.
Planned postoperative radiation, obesity, prior breast scars, and previous lumpectomy/radiation may increase the risk of complications, but they are not absolute contraindications to performing DTI reconstruction.
The breasts are assessed for volume, symmetry, nipple position, inframammary fold (IMF) position, and breast base width.
Patients with very small (less than 100 g) or very large (greater than 900 g) breasts are typically better candidates for tissue expander/implant reconstruction.
If a patient has asymmetry, a better cosmetic outcome may be achieved in two stages for bilateral reconstructions.
IMAGING
Preoperative mammogram or MRI can determine the oncologic safety of proceeding with a nipple-sparing vs skinsparing mastectomy based upon the proximity of the cancer to the nipple.
SURGICAL MANAGEMENT
Surgical management requires either a team approach with the surgical oncologist and plastic surgeon or an oncoplastic surgeon experienced in both mastectomy and reconstruction.
During the preoperative visit, patients are to be counseled on the possibility of a two-stage tissue expander/implant reconstruction or delayed reconstruction depending on the intraoperative mastectomy skin viability.
Though saline implants can be used, silicone implants are used more commonly to create a more nature look and feel.
Smooth round implants are softer than are anatomic implants and typically provide more superior pole fullness.
Textured anatomic implants are firmer than round implants and typically have reduced risk of rippling. These implants may better match a contralateral breast in unilateral reconstructions and may have less contracture after postmastectomy radiation.
Partial pectoralis muscle coverage of the implant is the most common technique with an inferior sling of ADM or synthetic mesh.
Compared to total muscle coverage, partial muscle coverage gives more natural breast shape and can accommodate a larger size implant.
Compared to no muscle coverage, partial muscle coverage has better soft tissue coverage in the upper pole, and it is less expensive.
Human ADM is the most common material used to provide an inferior sling.2 Alternative materials include porcine skin, bovine skin, and synthetic meshes made from silk, Vicryl, and titanium. These products provide precise control of the lateral and inframammary pocket borders along with the lower pole projection. They also support the implant and help keep the pectoralis muscle on stretch.
The authors describe their preferred technique using partial muscle coverage with an inferior pole sling of human ADM.
Preoperative Planning
A paravertebral block can be performed for perioperative and postoperative analgesia.
Reference markings are placed including the IMF bilaterally and planned lateral border of the breasts.
For skin-sparing procedures, the incision is placed around the areola, with or without small medial and lateral extensions.
For nipple-sparing procedures, an inferolateral IMF incision optimizes mastectomy, lymph node sampling, and reconstruction.
Alternative incisions in NSM include lateral radial, vertical, or extension of a nonradiated scar (FIG 1).
A full-thickness periareolar incision is typically avoided to decrease risk of nipple and skin loss.
Circumvertical mastopexy or Wise pattern mastopexy procedures at the time of mastectomy are associated with a higher risk of complications and are typically avoided.
The goal is for placement of an appropriate-sized implant within the pocket for uneventful wound healing and centralization of the nipple if preserved.
Positioning
The patient is placed in the supine position with arms extended, secured on arm boards, and angled to the side.
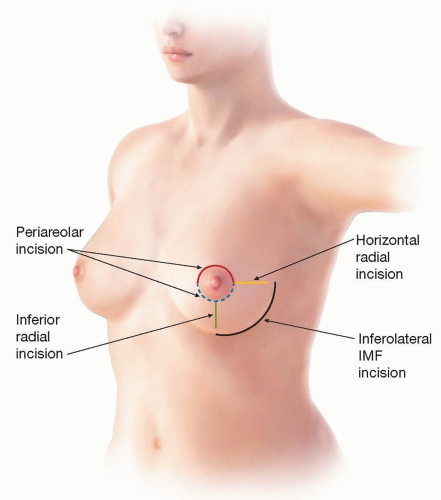
FIG 1 • Depending on tumor location and surgeon preference, these are the possible incision locations for nipple-sparing mastectomy.
Intraoperatively, the patient will be placed in the sitting position to assess size and symmetry before permanent implant placement.
Approach
Implant placement can be performed through any access incision used for the mastectomy.
For NSM, an inferolateral IMF incision is most commonly used and has excellent appearance.3
TECHNIQUES
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


