CHAPTER 56 Difficult breast augmentations
Tuberous breast deformity
Anatomy
• Breast hypoplasia mostly in the lower pole of the breast that can encompass the entire breast.
• Herniation of the breast through the areola.
• Constricting band around the breast.
The deformity is well described by Grolleau:
Physical evaluation
The key parts of the physical examination include:
Technical steps
The procedure to correct the tuberous breast includes the following options:
• Periareolar mastopexy in most cases.
• Soft tissue parenchymal manipulation to reshape the existing breast tissue.
• Breast augmentation, frequently asymmetric.
• Manipulation and lowering of the inframammary fold.
• Scoring the lower breast skin flap in the lower pole of the breast.
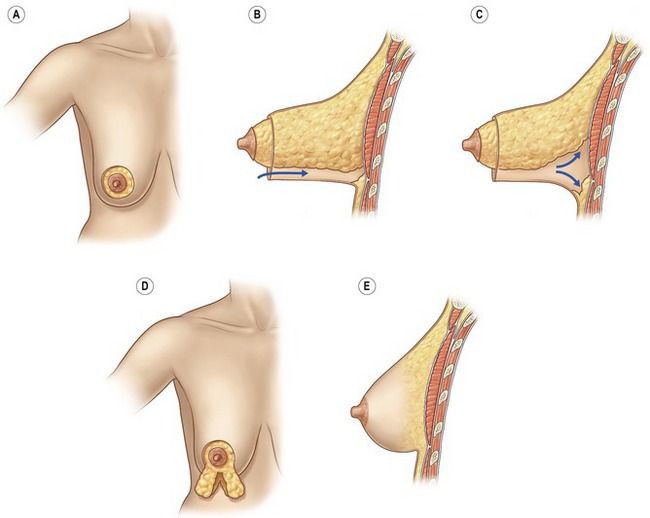
Periareolar mastopexy is almost always a part of any procedure to treat tuberous breasts. After the periareolar skin resection, a lower breast skin flap is elevated. The breast is completely mobilized to the chest wall and then the dissection is continued superiorly until the entire lower breast is mobilized and delivered through the incision. The breast is usually split at the 6 o’clock position and medial and lateral flaps are created. The fibrous ring is divided. Additional cuts are made in the ring if needed. The flaps are sutured together to make a round more normal lower pole of the breast (Fig. 56.1). If the skin of the lower pole of the breast is felt to be deficient, a tissue expander may be inserted. If need for a tissue expander is though to be a possibility, it should be discussed with the patient prior to surgery. In most cases, a tissue expander is not required and the breast is augmented. Usually a subpectoral or dual-plane pocket is created, a sizer is placed, and the appropriate implant is selected. The areola is closed with a permanent purse-string suture (Fig. 56.2).