Recognition of alar rim deformities is an important component of the preoperative analysis of the nose. Correction of these deformities improves the esthetic balance of the nose and has an added benefit of improving the function of the external nasal valve. Classification systems have been proposed to enable surgeons to more accurately diagnose alar deformities. These classification systems help guide surgeons as to the appropriate surgical procedure to correct a problem. The purpose of this article is to review the proposed classification systems for alar rim deformities and review the specific surgical techniques that have been proposed for each of the deformities.
Recognition of alar rim deformities is an important component of the preoperative analysis of the nose. Correction of these deformities improves the esthetic balance of the nose and has the added benefit, in some patients, of improving the function of the external nasal valve.
In recent years classification systems have been proposed, which enable surgeons to more accurately diagnose alar deformities. These classification systems help guide surgeons as to the appropriate surgical procedure to correct the problem. The purpose of this article is to review the proposed classification systems for alar rim deformities and review the specific surgical techniques that have been proposed for each of the deformities.
Classifications of alar rim deformities
Gunter and colleagues proposed a classification for alar-columellar discrepancies, which defines the normal alar columellar relationship based on a line drawn through the most anterior and posterior points of the nostril on the lateral view ( Fig. 1 ). The nostril represents an oval in which the alar rim forms the upper border of the nostril and the columellar rim, at the junction of the external skin with the vestibular skin, forms the lower border of the nostril. This oval is occasionally interrupted by flaring of the feet of the medial cura, but this should be disregarded when analyzing the relationship. In a normal alar-columellar relationship, the greatest distance from the long axis of the nostril to the alar rim or the columellar rim should be 1 to 2 mm.
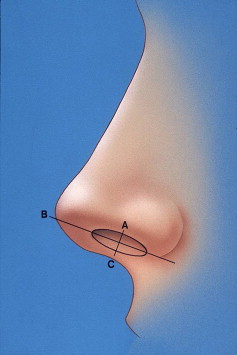
A hanging ala results in decreased columellar show with the distance between the long axis of the nostril and the alar rim being less that 1 to 2 mm. A retracted ala is characterized by an alar rim to nostril long axis distance of more than 2 mm. The true “hanging columella” occurs when the distance between the long axis of the nostril and the columellar rim is greater than 2 mm and the distance from the long axis to the superior nostril rim is the normal distance of 1 to 2 mm. It is important not to misdiagnose a hanging columella as a retracted ala. A retracted columella is characterized by the distance between the columellar rim and the long axis of the nostril less than 1 to 2 mm.
Of the four basic deformities (defined previously), retracted ala, hanging ala, retracted columella, and hanging columella, only the retracted ala and the hanging ala represent true alar rim deformities. Of these two, the retracted ala is the deformity that has generated the most interest from surgeons attempting to correct it.
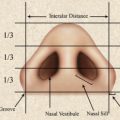
Guyuron subsequently expanded the classification of alar rim deformities to include an analysis from the perspective of the alar basilar view, in contrast to Gunter’s classification, which focused on the alar columellar relationships in the lateral (profile) view. In the ideal basal view, the alar rim anatomy forms an equilateral triangle. The ala forms a straight line, which constitutes two sides of the triangle, with the alar base width forming the third side. Guyuron recognized two distinct alar abnormalities, the concave and the convex ala. The concave ala is defined as the lateral border of the ala being medial to the line of the equilateral triangle. The convex ala is defined as the lateral border of the ala extending lateral to the line of the equilateral triangle.
Treatment of alar rim deformities
For the purposes of this discussion, the treatment of alar deformities is divided into deformities seen in the lateral (profile) and those seen in the basilar view.
Lateral View Alar Deformities
The hanging ala
The most common technique to correct a hanging ala is to excise an ellipse of vestibular skin. The ellipse should be horizontal and parallel to the alar rim. The width of the ellipse should be slightly more than the planned elevation of the alar rim ( Fig. 2 ). Care should be taken not to excise too much to avoid a rolled in appearance of the alar rim, so the excision should not exceed 3 mm. Other options for raising the ala include excision of skin of the nose, trimming of the cephalic or caudal border of the lateral crus and excision of nasal lining. Direct excision of skin at the alar rim is best performed in patients with thick sebaceous skin but may lead to visible scarring. This is rarely used because of the scar. McKinney and Stalnecker found resection of the caudal border of the lateral crus to be useful in thin-skinned patients and has resected up to 2 mm. The trimming of the caudal border must be accurate and smooth to prevent any irregularity or notching of the alar rim. This technique does not work well in thick-skinned patients because the skin is not pliable enough to conform to the new position of the cartilage. Excision of the nasal lining in the area of the cephalic border of the alar cartilage is effective in thick-skinned patients. Caution is advised, however, because the resection must be caudal to the internal nasal valve and in general over-resection of lining should be avoided.
Another option for raising the alar rim is direct excision of the ala. This can be done by excising the skin and mucosa and then undermining the skin edge and advancing it to close it to the mucosa. Millard had also proposed alar margin sculpturing in a thick hanging ala. Irregularities and scarring of the alar rim may result so direct excision is used less often than other techniques.
The retracted ala
The correction of a retracted ala depends on the severity of the retraction. If only a small amount of lowering is desirable, an alar base resection provides some lowering of the alar rim. If the retraction is mild, the deformity can be corrected by separating the lateral curs from the accessory cartilage and moving the cartilage caudally. This is only effective if there are no associated tissue deficiencies.
For moderate alar retractions, cartilage grafting may be more appropriate. Rohrich and colleagues have described the alar contour graft for correction of alar rim deformities. This technique is done with an open approach. Using the medial end of the infracartilaginous incision, a pocket is undermined cephalic and parallel to the alar rim. A cartilage graft of approximately 5 mm by 25 mm is used, or at least long enough to span the retracted area. The graft is placed in the pocket and stabilized to the nasal lining medially with one 5-0 plain gut suture. Septal cartilage is the first choice for grafting, but auricular cartilage is an acceptable second choice. This technique can also be used with a closed approach. An incision is made in the posterior vestibule perpendicular to the rim, and a tunnel is developed along the rim and the graft is inserted.
An alternative to the alar rim graft when using an open approach is to place a cartilage graft caudal to the existing lateral curs. To facilitate this, the vestibular incision is made caudal to the caudal rim of the lateral curs, thus leaving a cuff of vestibular skin below the lateral curs. The graft is placed in a pocket under this cuff of vestibular skin.
For more severe alar retraction, a lateral crural strut graft may be indicated ( Fig. 3 ). This is a versatile technique, which can be used to treat other alar deformities, such as alar rim collapse, and concave lateral crura, in addition to correction of alar retraction. This is also done with an open rhinoplasty technique. The vestibular skin is dissected from the cephalic border of the crura toward the caudal border. The vestibular skin is left attached to the caudal border. The lateral crura are separated from the accessory cartilages. A cartilage graft measuring 3 to 4 mm in width and 15 to 25 mm in length is fashioned from septal cartilage, but auricular or rib cartilage can also be used. A longer strut is indicated for the correction of alar retraction. The pocket is made in the soft tissue below the alar groove, and the lateral end of the strut is placed in the pocket, thus positioning the lateral crura more caudally. This is technically more demanding than the alar contour graft and is indicated for more severe cases of alar retraction or secondary cases.
A modification of the lateral crural strut is the intercartilaginous graft for moderate to severe alar retraction as described by Gruber and colleagues ( Fig. 4 ). The graft is placed between the upper lateral cartilage and the lateral crus or the remnant of the lateral curs. This lengthens the lateral nasal sidewall. Key to this procedure is soft tissue release between the lateral crus remnant and the upper lateral cartilages. Scissors are used the spread between the two, while attempting to preserve the vestibular mucosa. A gap of 4 mm and up to 8 mm may be made with the soft tissue release. The release often results in some undermining of the vestibular skin of the lateral crus. The septal graft is placed between the upper lateral cartilage and the lateral curs and is sutured to the upper lateral cartilage and under the upper edge of the lateral curs.
The traditional treatment for severe alar retraction in patients with scarring or lining deficiencies is composite grafting, usually with septal cartilage and mucosa or auricular cartilage and skin ( Fig. 5 ). A vestibular incision is made parallel to the rim with inferior mobilization of the rim by releasing the soft tissue with scissors. The composite graft is placed in the resulting defect. The graft is sutured to the defect and may be stabilized with a bolster dressing for 1 week.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


