18 Diabetic Foot Reconstruction
Summary
The treatment of diabetic foot ulceration is complex with multiple considerations and unfortunately often leads to amputation. A multidisciplinary approach along with an algorithm to manage and salvage diabetic foot ulcers from amputation is now a highly doable approach. Knowing the spectrum of care and reconstructive principles can prevent diabetic foot ulcers from amputation. Further understanding of supermicrosurgery and angiosome principles can extend the possibility for reconstruction in patients with severe ischemic diabetic foot.
Keywords: diabetic foot, supermicrosurgery, angiosomes, diabetic foot reconstruction
18.1 Introduction
According to the statistics given, approximately 3 to 4% of individuals with diabetes currently have foot ulcers or deep infections and 25% will develop foot ulcers sometime during their lifetime.1,2 The risk of lower leg amputation increases by a factor of 8 once an ulcer develops. It is estimated that the age-adjusted rate of lower extremity amputation in diabetic patients is 15-fold that of nondiabetic patients.3 Intractable diabetic foot ulcers can not only cause decreased physical, emotional, and social functions but also be a huge economic impact to the patient.4,5,6 Furthermore, the 5-year mortality after major amputations may range from 39% to as high as 80%.1,7,8 These are the reasons why salvage for diabetic foot ulcers remains important as it will reduce economic burden and improve the quality of life.8
Limb salvage from diabetic foot using the microsurgical approach showed similar success comparable to nondiabetic patients.9,10,11,12,13,14 Meta-analysis of a systematic review of free tissue transfer in 528 diabetes patients in 18 studies showed flap survival of 92% and limb salvage rate of 83.4% over a 28-month average follow-up period. This study indicates that free tissue transfer in the management of nontraumatic lower extremity wounds in patients with diabetes may avoid amputations.13 Free flaps and microsurgery technique now play an important role to salvage the limb from chronic ulcerations. A previous study showed that using microsurgery can achieve an overall limb salvage rate of 84.9% and 5-year survival of 86.8%.8 There is no doubt that a well-vascularized free flap will enhance healing, quality of life, and survival chances.
In this chapter, we will focus on the clinical aspect of reconstruction and show a step-by-step approach on how to achieve reconstructive goals.
18.2 Attributes and Detriments
18.2.1 Attributes
• Limb salvage using reconstruction is an alternative to amputation.
• A multidisciplinary approach is essential in managing diabetic foot ulcers as diabetic patients have high comorbidity.
• Once good vascular supply is secured, microsurgical or local reconstruction can be performed with reliable outcome.
• The key is the status of the recipient artery and supermicrosurgery approach using small vessels can be considered.
• Limb salvage not only leads to better quality of life but may also increase 5-year survival.
18.2.2 Detriments
• A multidisciplinary approach is needed to adequately obtain good systemic condition and vascularity for reconstruction and may not be readily available.
• Learning curve is needed to understand the algorithm of reconstruction and care.
18.3 Considerations
18.3.1 Multidisciplinary Approach and Spectrum of Care
The spectrum of diabetic foot disease may vary from asymptomatic to critically ischemic limb with unavoidable amputation. The spectrum of care for diabetic foot patients ranges from managing blood glucose, education on prevention, and managing small ulcers with good standard of care to using multiple new techniques and approaching with surgery (▶ Fig. 18.1).15 The wide manifestation of symptoms is due to multifactor pathophysiology. The principal pathogenesis involves ischemia, neuropathy, and infection. The addition of external trauma, peripheral edema, and foot deformity may further increase the risk for diabetic foot ulceration.16 They may act alone or synergistically to result in Charcot’s deformities, Achilles tendon contractures, ulcerations, necrosis, and gangrene. One must consider these pathologies and manage them in sequence in order to provide an efficient care for the foot. Treatment must begin with strict blood sugar control and nutritional support while aggressively managing the wound and infection to achieve closure of the defect.17 In the cases with ischemic limb, vascular bypass or angioplasty may play a vital role to enhance circulation allowing further reconstruction of soft tissue and bone.15
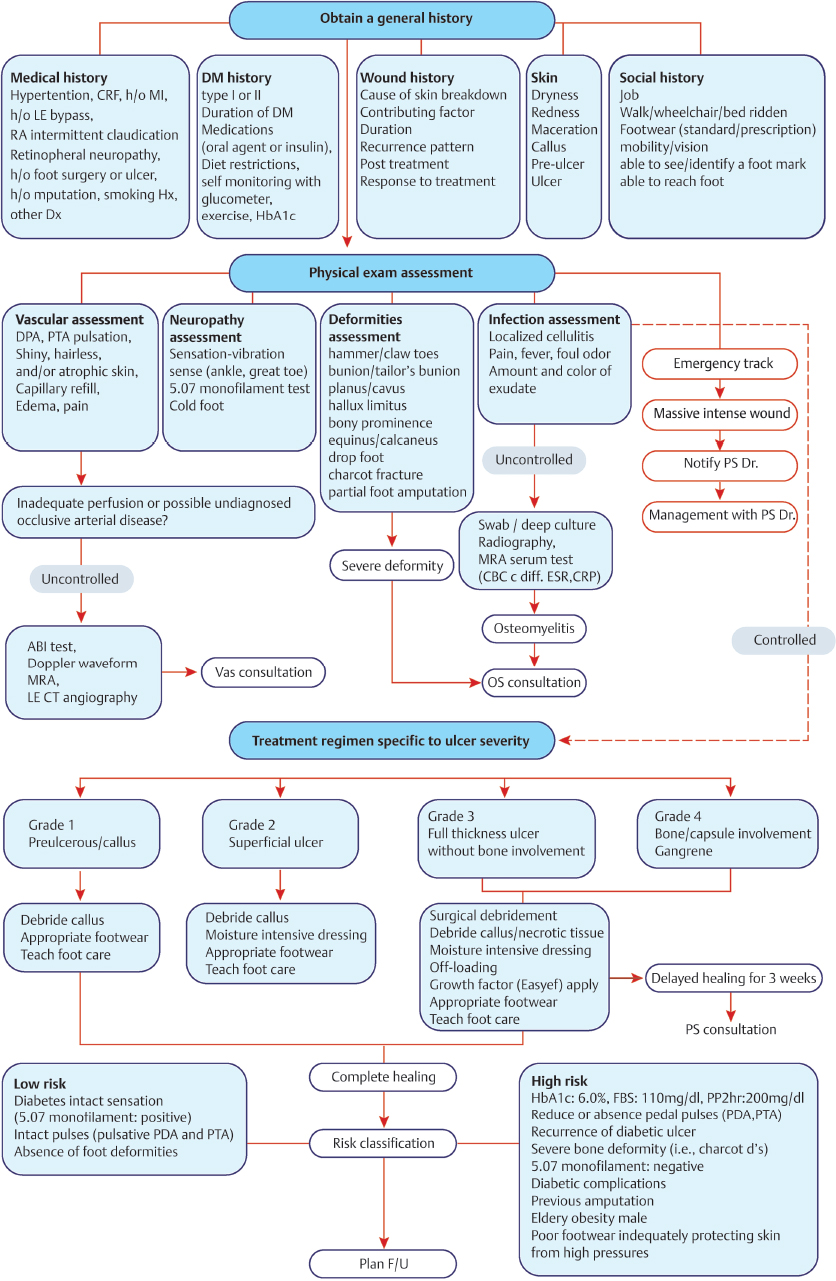
The nurse specialist or coordinator helps use the team recourses efficiently. After gathering general information about the patient and initial screening of the systemic and foot condition, the specialist would refer to an endocrinologist, nutritionist, and proper departments for further treatment and evaluation. There are four categories for initial foot evaluation: vascular, neuropathic, orthopaedic, and infectious wounds.15 Multiple departments may be involved simultaneously to improve the patient’s foot condition. In the cases of emergent wound, a dedicated team needs to be notified immediately for emergency debridement and further clinical decision. This is the first and a major step to limit the spread of acute infection that may be critical in salvaging the diabetic foot.18▶ Fig. 18.2 shows the multidisciplinary algorithm for primary screening and initial treatment for wounds.15
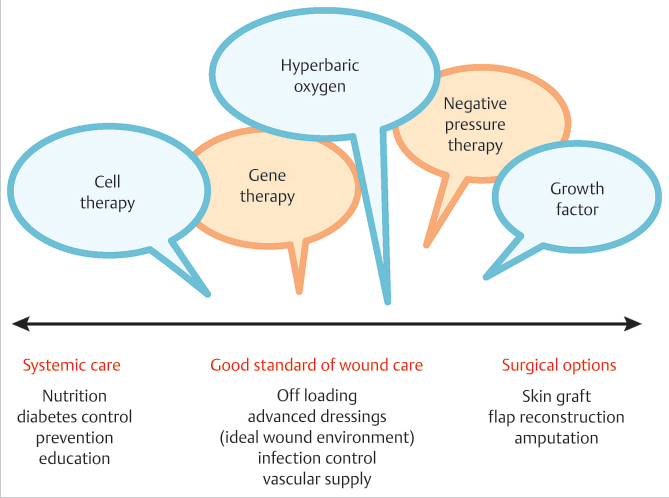
Fig. 18.1 Treating diabetic foot requires a multidisciplinary care as the spectrum of care is very wide from managing blood glucose, education on prevention, and managing small ulcers with good standard of care to using multiple new techniques and approaching with surgery.
With the introduction of the multidisciplinary approach, the trend of management has shifted from major amputation to limb salvage.19 Addressing the issues of perfusion, infection, wound treatment, off-loading, and bone surgery, we are able to increase the salvage rate. Similar with other reports, the major amputation rate for diabetic foot in our center has reduced significantly after a multidisciplinary approach and recently maintains to be about 3 to 4%.20,21 Although the indications for major amputation still exist and are often caused by multiple factors such as systemic sepsis, major tissue loss, significant comorbid factors, poor patient compliance, and non-reconstructable peripheral vascular disease, the goal remains the same: to salvage the limb under good clinical judgment. A nonhealing ulcer itself should not be considered an indication for amputation but be explored to solve the pathology behind it.15,22,23
18.3.2 Role of Microsurgery
Till recently, reconstruction with microsurgical techniques has been under debate.15 This was due to the incorrect “myth” that patients with diabetes have an increased incidence of small-vessel disease that results in foot ulcers. Particularly, it was felt that patients with diabetes have arteriolar occlusive disease, which can cause ischemic lesions. This concept was first attributed to Goldenberg et al in 1959.24 They studied amputation specimens from patients with gangrene and concluded that diabetic patients have endothelial hypertrophy and proliferation in the smaller arteries, with complete occlusion of the lumen in several cases. But subsequent studies have failed to demonstrate increased arteriolar occlusive disease or endothelial proliferation.25,26,27 A thickening of the capillary basement membrane has been documented, but capillary narrowing or occlusion has not been documented.25 The same study showed that diabetics often have atherosclerotic occlusion of the tibial arteries, but the occlusive disease occurs mainly in the leg so that the arterial system in the foot is less involved. Also as the patient undergoes obstruction of major vessels, new collateral sprouts to maintain a relatively stable vascularity to the foot.28 Based on these studies, limb salvage from diabetic foot using microsurgical approach showed similar success in nondiabetic patients.9,10,11,12,13,14 Meta-analysis of a systematic review of free tissue transfer in 528 diabetes patients in 18 studies showed flap survival of 92% and limb salvage rate of 83.4% over a 28-month average follow-up period. This study indicates that free tissue transfer in the management of nontraumatic lower extremity wounds in patients with diabetes may avoid amputations.13 Free flaps and microsurgery technique now play an important role to salvage the limb from chronic ulcerations.8,10,15,29,30
18.4 Surgical Algorithm
While the medical care for the patient with diabetic foot ulceration begins with stabilization of the patient’s systemic condition including blood glucose, the surgical care begins with debridement and control of infection. After the patient and the wound stabilized, further evaluation of the wound is made. Unless indicated for major amputation, the reconstructive algorithm is followed as shown in ▶ Fig. 18.3.15 If it is a simple wound with minimal or no vital structures exposed, conservative care with various treatments can be considered. If well granulating after wound preparation, skin graft or a small local flap can be performed.31 Well-granulating wounds can be an indication for good vascularity. However, if healing is stalling, then further evaluation using transcutaneous oxygen pressure measurement (TcPO2) or angiograms are warranted to evaluate the arterial flow and prepare for vascular intervention. The same evaluation and approach to ensure vascularity are needed for complex wounds waiting reconstructive procedure.
Related posts:
 General Wound Preparation and Timing
General Wound Preparation and Timing
 The Pertinence of the Reconstructive Ladder and the Reconstructive Elevator
The Pertinence of the Reconstructive Ladder and the Reconstructive Elevator
 Supermicrosurgery Approach to the Lower Limb
Supermicrosurgery Approach to the Lower Limb
 Lower Limb Vascularized Composite Allotransplantation
Lower Limb Vascularized Composite Allotransplantation
 Using the Flap and Angiosome Concepts to Optimize Functional Lower Leg and Foot Amputations
Using the Flap and Angiosome Concepts to Optimize Functional Lower Leg and Foot Amputations
 Procurement of Thin Flaps as Indicated in the Lower Extremity
Procurement of Thin Flaps as Indicated in the Lower Extremity
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


