Key Words
Mohs, excision, lasers, electrodessication, curettage, cryosurgery, botox, fillers, liposuction, cosmetic
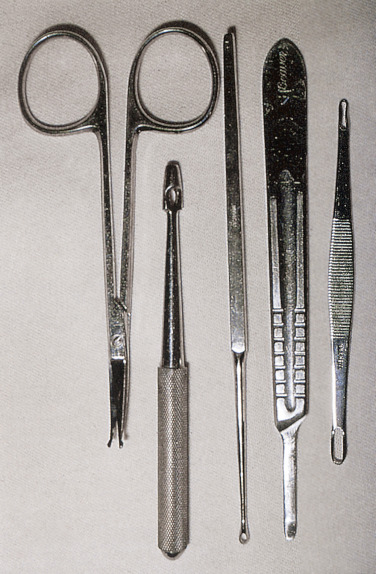
Punch biopsy, shave biopsy, electrodesiccation and curettage (ED&C), blunt dissection, and simple excision and suture closure are the basic techniques that should be learned by physicians who treat skin disease. One should be familiar with the more sophisticated techniques, such as Mohs micrographic surgery, so that referral to physicians who perform these techniques can be made at the proper time. The instruments used for most basic dermatologic surgical procedures are shown in Fig. 27.1 .
Antibiotic Prophylaxis
- •
Antibiotics are not helpful in treating cutaneous abscesses, inflamed epidermal cysts, uninfected atopic eczema, and cutaneous ulcers caused by venous insufficiency or diabetes in the absence of significant contiguous soft tissue inflammation.
- •
Prophylactic antibiotics are rarely appropriate for routine dermatologic surgery and are not indicated for patients who have prosthetic joints or vascular grafts.
- •
Topical antibiotics are no better than white petrolatum in covering sutured wounds, and with moist occlusive dressings, no ointment is necessary.
For patients with high-risk cardiac conditions, and a defined group of patients with prosthetic joints at high risk for hematogenous total joint infection, prophylactic antibiotics are recommended when the surgical site is infected or when the procedure involves breach of the oral mucosa. For the prevention of surgical site infections, antibiotics may be indicated for procedures on the lower extremities or groin, for wedge excisions of the lip and ear, for construction of skin flaps on the nose or skin grafts, and for use in patients with extensive inflammatory skin disease.
- •
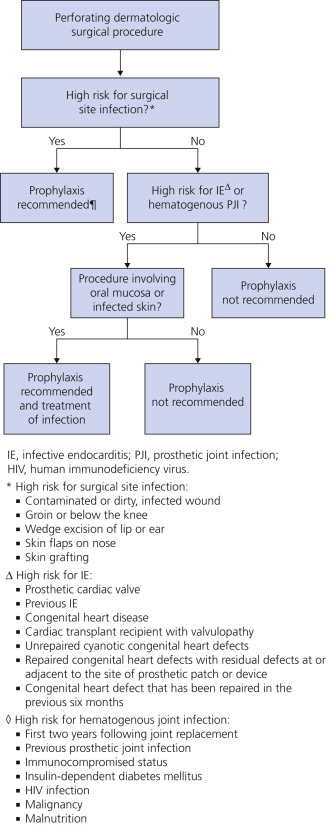
The first step in determining the need for antibiotic prophylaxis in dermatologic surgery is assessment of the risk of surgical site infection and aggressive treatment of any cutaneous infection in patients with joint or valve replacements.
- •
Perforating dermatologic surgery involves invasion of or immediate destruction of the epidermis or mucosa and includes excision, Mohs micrographic surgery, biopsy, ablative laser, incision and drainage, and ED&C. Nonperforating dermatologic surgical procedures, such as cryotherapy and nonablative laser, are not an indication for prophylaxis.
- •
Oral mucosa is defined as portions of the nonglabrous oral tissue posterior to the junction where closed lips meet.
- •
Patients with low-risk cardiac indications do not receive antibiotic prophylaxis for oral procedures but receive therapeutic antibiotics for an infected site. Examples of patients who would not routinely receive antibiotic prophylaxis for infective endocarditis include those with pacemakers, defibrillators, peripheral vascular stents, vascular grafts, coronary artery stents, breast implants, penile prostheses, and central nervous system shunts.
- •
Antibiotics are not indicated in patients with orthopedic pins, plates, or screws and not in the majority of healthy patients with a total joint prosthesis.
Mohs Micrographic Surgery – Indications for Antibiotics
The routine administration of prophylactic antibiotics for Mohs micrographic surgery is not recommended. With the low rate of bacteremia during Mohs surgery, prophylaxis against infective endocarditis and hematogenous total joint infection is usually not indicated. For patients who are at high risk for surgical site infection based on the site or technique used, antibiotic prophylaxis should be given. For patients at high risk for infective endocarditis or hematogenous total joint infection, if the surgical site includes oral mucosa, antibiotic prophylaxis is indicated. If the site is infected before the procedure , aggressive treatment should be initiated, cultures ascertained, and prophylaxis for infective endocarditis or hematogenous total joint infection also given. Mohs surgical cases are heterogeneous, and some may involve breach of nasal mucosa or may extend over many hours; each patient’s clinical scenario should be considered individually and prophylaxis decisions should be made after taking into account all relevant factors. As the risk of surgical site infection increases and the potential morbidity following an infection increases, the threshold for antibiotic prophylaxis should decrease.
Local Anesthesia
Lidocaine (Xylocaine) 1% or 2%, with or without epinephrine, is used for most surgical procedures. The onset of anesthesia is almost instantaneous, and the duration is adequate for most minor procedures. A 27-gauge or, preferably, a 30-gauge needle is used.
Epinephrine.
The vasoconstriction induced by epinephrine prevents absorption of lidocaine, prolongs anesthesia, and controls bleeding. Lidocaine with epinephrine is safe for distal digits, penis, ears, and toes, but should not be administered for digital blocks, where complete blood flow to the digit could be compromised.
Lidocaine Allergy.
Allergy to lidocaine is very rare. Most patients who claim to be allergic have had a vasovagal response. Bacteriostatic saline is an alternative for patients who are allergic to lidocaine (see the following discussion).
Pain Reduction.
Anesthetics produce a sharp pain during skin infiltration. Pain is greater with rapid injections and can be minimized with slow injections through a 30-gauge needle. The needle should be inserted slowly but firmly into the dermis. A needlestick at 90 degrees to the skin surface causes less pain because fewer nerves are transversed by the needle. The skin is rapidly pinched between the thumb and forefinger and shaken just before and during the injection. Pinching the skin in the area to be injected either distracts the patient or blocks the transmission of pain impulses caused by the injections. Placing the needle distal to the area of pinched skin is more effective. Anesthesia is initiated by injecting a tiny amount of fluid; after a few seconds, infiltration is continued slowly until the skin surrounding the lesion blanches. A wheal can be raised by inserting the needle almost vertically. Penetration of the thick palm and sole skin is very painful. The area about the nostrils is very sensitive. Intrafollicular injection into the large follicles of the nose and cheeks minimizes pain. Superficial injections into the penis and vulva are well tolerated.
Painless Anesthesia.
Icing the lesion for 1 minute numbs the skin and minimizes needle-penetration pain. Adequate anesthesia with little or no infiltration pain can be induced with the following preparations. Bacteriostatic saline and lidocaine diluted with bacteriostatic saline solution injections are less painful than 1% lidocaine with sodium bicarbonate. It is unlikely that the pain of infiltration is a simple function of the pH of the anesthetic solution.
Bacteriostatic Saline.
Commercially available bacteriostatic saline contains benzyl alcohol, which acts as a painless anesthetic. The anesthetic effect dissipates rapidly when injected subcutaneously. The volume of saline required to achieve anesthesia is at least two to three times that required when using 1% lidocaine and is of brief duration.
Saline and Epinephrine.
The addition of 3 mL of epinephrine 1 mg/mL (1 : 100,000 diluted) to 30 mL of bacteriostatic saline extends the duration of anesthesia from 4 minutes to 120 minutes. Bacteriostatic saline should not be used as an anesthetic for newborns.
Saline Diluted With Lidocaine.
A mixture of saline (27 mL) and lidocaine 1% with or without epinephrine (3 mL) is also effective.
Buffered Lidocaine.
The addition of sodium bicarbonate (NaHCO 3 ) reduces the pain produced by infiltration of lidocaine with or without epinephrine. One milliliter of NeutraCaine, a 7.5% sodium bicarbonate buffer solution, is added to 5 mL of lidocaine or bupivacaine. Buffered lidocaine and epinephrine maintain greater than a 90% concentration 2 weeks after buffering when stored at 0 to 4° C. This permits batch buffering and storage for up to 2 weeks when properly refrigerated. NaHCO 3 enhances the killing effect that has been described for lidocaine alone. The inability to recover common pathogenic bacteria from biopsy specimens could be the result of exposure to lidocaine buffered with NaHCO 3 . Warming the local mixture to 40° C reduces the discomfort of injection even further.
The Ice–Saline–Lidocaine Technique.
This is a simple method of minimizing pain when obtaining local anesthesia. Cryo-Gel packs are applied before the local anesthetic injection to minimize the pain of piercing the skin with the injection needle. The surgical field is then infiltrated with benzyl alcohol–containing normal saline. Subsequently, lidocaine with epinephrine can be infiltrated without discomfort.
EMLA, ELA-Max.
EMLA is a mixture of 2.5% lidocaine and 2.5% prilocaine in an oil and water emulsion. ELA-Max is a topical anesthetic cream with 4% lidocaine at pH 7.4. These agents should be applied to the desired area for approximately 1 hour under an occlusive dressing. They provide effective analgesia, making them useful for superficial surgery, split-thickness skin grafts, venipuncture, argon laser treatment, epilation, and debridement of infected ulcers. Other indications have included use in postherpetic neuralgia, hyperhidrosis, painful ulcers, and inhibition of itching and burning. A single application of ELA-Max in children weighing less than 10 kg or between 10 and 20 kg should not be applied over an area larger than 100 cm 2 .
Hemostasis
Monsel’s solution (ferric subsulfate) is a valuable agent for providing rapid hemostasis. It is particularly effective in controlling bleeding after curettage of seborrheic keratosis and basal cell carcinoma (BCC). Immediate hemostasis is most efficiently achieved if the solution is applied when the wound is not bleeding. To exert tension and stop bleeding, the thumb and index finger are placed at the opposite edges of the wound, and the skin is stretched. The blood is then wiped with gauze, the Monsel’s solution is applied with a cotton-tipped applicator, and the tension is maintained for approximately 15 seconds. The lack of blood flow apparently allows more complete coagulation.
Monsel’s Artifact.
When a biopsy is repeated, an area of skin that has been treated with Monsel’s solution has a pigmented artifact that can interfere with histologic interpretation. The use of Monsel’s solution should be avoided after biopsies of pigmented lesions or tumors that may prove to be diagnostic problems. The pathologist should be informed if Monsel’s solution has been used.
Wound Healing
Types of Cutaneous Wounds
Full-Thickness Wounds.
In full-thickness wounds, the epidermis and the full thickness of the dermis are lost. The defect is deeper than the adnexa (hair follicles, eccrine sweat ducts). These wounds heal by contraction (associated with myofibroblast development), granulation tissue formation (with fibroplasia and neovascularization), and reepithelialization. Contraction causes a 40% decrease in the size of the wound. Epithelialization occurs from the wound edges.
Partial-Thickness Wounds.
In partial-thickness wounds, the epidermis and some portion of the dermis with parts of the adnexa remain in the wound bed. Such wounds are produced by shave excisions, ED&C, dermabrasion, chemical peels, and carbon dioxide (CO 2 ) laser surgery. These wounds heal quickly through reepithelialization from the wound edges and adnexal structures in the base of the wound. Wound contraction is minimal when only the most superficial portion of the dermis has been lost.
Physiology of Wound Healing
The acute phase of wound healing takes 3 to 14 days and has three phases: inflammation, proliferation, and remodeling with wound contraction ( Fig. 27.3 ). The inflammatory phase begins as neutrophils and macrophages appear. The proliferative phase involves the formation of a collagen matrix and granulation tissue and then epidermal cell migration over the matrix. The remodeling phase sees fibroblasts evolve to compact and contract the wound. Wounds gain about 20% of their final strength in the first 3 weeks. Protein or vitamin deficiencies may impair collagen production, and necrotic tissue in the wound bed may impede reepithelialization.
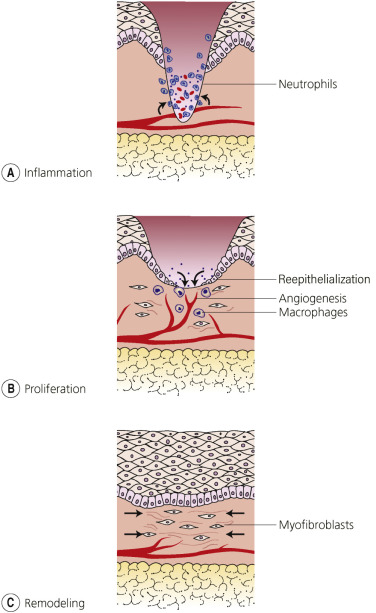
Inflammatory Phase.
Neutrophils appear in a wound 6 hours after the event, reach their greatest number after 24 to 48 hours, and start to disappear after 72 hours. Aggregated platelets and damaged cells secrete chemical mediators to attract and activate inflammatory cells and fibroblasts. Vasodilation and increased permeability of local capillaries permit neutrophils to move into the wound site to phagocytize bacteria and debris.
Proliferative Phase.
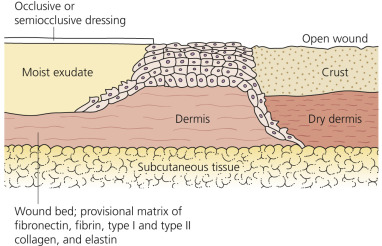
Activated macrophages release vascular endothelial growth factor (VEGF) to stimulate granulation tissue formation. Fibroblasts populate the wound after 48 to 72 hours. Fibroblasts produce a collagen matrix, new blood vessels invade the forming granulation tissue, and epidermal cells migrate across the wound surface to close the wound. Keratinocytes initially migrate over a matrix of fibrin, collagen, and elastin. This matrix acts as a structural support for cell migration. Epidermal migration and proliferation occur from the epithelial cells at the edge of the wound and from appendageal structures remaining in the wound bed. The rate of reepithelialization is directly related to the moistness of the wound. Open, dry wounds reepithelialize slower than occluded, moist wounds. The migration of keratinocytes beneath a dry crust is slower than the migration over an occluded, moist wound, where the plane of epithelial cell migration lies near the wound surface ( Fig. 27.4 ). Protein or vitamin deficiencies may impair collagen production, and necrotic tissue in the wound bed may impede reepithelialization.
Remodeling.
Wounds gain about 20% of their final strength in the first 3 weeks of normal wound healing through collagen deposition, remodeling, and wound contraction. Fibroblasts remodel the collagen matrix. Wound contraction begins at 1 week after the wound occurs. Myofibroblasts are modified fibroblasts that resemble smooth muscle cells. They contain large amounts of contractile proteins and are responsible for wound contraction.
Tensile strength in a wound increases progressively up to 1 year after the wound occurs. Tensile strength in a healed wound is always less than 80% of normal. Healing time is related to the logarithm of the area. The width of the wound is a better predictor of healing time than is the area in which the wound occurred. Wounds created by destructive techniques (e.g., cryosurgery, electrosurgery, laser surgery, and chemical cautery) heal more slowly than clean wounds created by scalpel or curette surgery.
Normal Wound Healing
Wound management guidelines are listed in Box 27.1 .
- 1.
Use antiseptics for disinfection of intact skin only.
- 2.
Select a method of wounding that minimizes tissue necrosis.
- 3.
Use pinpoint electrocoagulation, pressure, topical thrombin, collagen, or gelatin rather than caustic agents to establish hemostasis.
- 4.
To prevent wound infection and to accelerate healing, apply topical antibiotics to the wound instead of antiseptics.
- 5.
Substitute tap water for hydrogen peroxide to cleanse wounds.
- 6.
Use nonadherent occlusive dressing on wounds to accelerate healing.
Impairment of Wound Healing
Topical Therapy.
Topical steroids may interfere with healing because of their antiinflammatory action ( Table 27.1 ).
| Agents | Relative Rate of Healing (%) * |
|---|---|
| Triamcinolone acetonide ointment (0.1%) | −34 |
| Furacin | −30 |
| USP petrolatum | −8 |
| Eucerin | +5 |
| Benoxyl lotion base (benzoyl peroxide preparation) | +14 |
| Silvadene cream | +28 |
| Neosporin ointment | +28 |
| Telfa dressing | +14 |
Antiseptic Solutions.
One percent povidone–iodine, 3% hydrogen peroxide, and 0.5% chlorhexidine solutions are toxic for fibroblasts and keratinocytes and may delay the formation of granulation tissue.
Hemostatic Solutions.
Monsel’s solution (ferric subsulfate), 30% aluminum chloride, and silver nitrate produce tissue necrosis and delay reepithelialization. The effect on small wounds is minimal.
Contact Dermatitis
Contact allergic reactions may occur with tapes and antibiotic ointments. Neomycin is a common sensitizer. Polysporin and bacitracin are not common sensitizers.
Systemic Factors.
Malnutrition interferes with healing. Vitamin C and zinc deficiencies lead to poor healing. Systemic steroids in a dosage greater than 10 mg a day interfere with healing. Clinical experience suggests no impairment of wound healing for patients taking chemotherapeutic drugs.
Wound Dressings
Wound Dressings – Mechanism of Action.
Occlusion of wounds leads to faster healing. The process of neovascularization within granulation tissue is stimulated by hypoxic conditions such as those that occur beneath occlusive, oxygen-impermeable dressings. Occlusive dressings prevent crust formation and drying of the wound bed. The rate of epithelialization is faster under occlusive dressings. Wound fluid under occlusive dressings is favorable to fibroblast proliferation. Adhesive occlusive dressings may remove newly formed epithelium. Hydrocolloid adhesive occlusive dressings prevent entry of bacteria into the wound. The use of occlusive dressings in chronic wounds leads to less pain, better granulation tissue, and painless wound debridement. In acute wounds, occlusive dressings promote bacterial growth but result in faster reepithelialization. There are numerous dressings available. These are routinely used in wound care clinics where complicated venous and arterial ulcers are treated.
Function.
Protection with dressings exerts pressure and maintains a moist wound environment. Dressings reduce pain when applied to partial-thickness wounds. Topical antimicrobial agents that may enhance reepithelialization include neomycin, polymyxin B, Neosporin ointment, silver sulfadiazine, and 20% benzoyl peroxide lotion. Hexachlorophene, chlorhexidine, and alcohol may retard reepithelialization.
Occlusive Dressings.
Crust formation is suppressed if the surface of the wound is kept moist by an occlusive film or by gauze applied over antibacterial ointments such as Neosporin (bacitracin, neomycin, and polymyxin B) or petrolatum. The level of adequate tissue humidity is then very close to the skin surface, and the epidermis migrates rapidly over the moist bed. Patients treated with occlusive dressings tend to have softer, smoother, smaller, and more superficial scars. There does not seem to be an increased incidence of infection with occlusive dressings. Occlusive dressings reduce wound pain. So-called oxygen-permeable membranes do not seem to transmit oxygen to the wound. Many synthetic occlusive dressings are available for a variety of wounds (see Chapter 3 ); examples of clinical uses include the following:
- •
Arterial and venous catheter sites
- •
Burns
- •
Decubitus ulcers
- •
Dermabrasion site after tattoo removal
- •
Leg ulcers following pinch grafts
- •
Mohs micrographic wounds
- •
Skin graft donor sites
- •
Stasis ulcers
- •
Surgical incisions
- •
Traumatic wounds
Postoperative Wound Care
Partial- and Full-Thickness Open Wounds
- 1.
Avoid alcohol and aspirin in the immediate postoperative period.
- 2.
Keep wounds covered and moist (e.g., with Polysporin or bacitracin) to prevent crusts.
- 3.
Bathing of granulating wounds is allowed. Avoid cleansing with hydrogen peroxide or povidone–iodine.
- 4.
Undressed sutured wounds can be washed with soap and water twice a day starting the morning after surgery.
Sutured Wounds
Office
- 1.
Semipermeable tape strips (e.g., Steri-Strips, Clearon skin closures) reduce tension across the suture line. Spaces left between the strips allow wound exudate to escape and to be absorbed by the overlying dressing.
- 2.
A nonadherent primary dressing may then be applied, taped in place, and covered with a pressure dressing applied (bulky gauze) and secured by adhesive tape.
- 3.
Tissue adhesives (tincture of benzoin, Mastisol) are applied to the skin to increase the adherence of tape to the skin.
- 4.
Pressure dressings (applied for 24 to 36 hours) reduce the risk of hematoma formation following the excision of cysts.
Home.
Small wounds do not require dressing for more than 24 to 48 hours.
- 1.
Change dressing once or twice daily. The dressing may be left in place for uncomplicated dry wounds until the sutures are removed.
- 2.
Cleanse with a mild liquid soap, sterile saline, or hydrogen peroxide solution.
- 3.
An antibiotic ointment (e.g., bacitracin) is applied and the wound is covered with a nonadherent dressing. The antibiotic ointment reduces the risk of the contact layer of the dressing adhering to the wound bed.
- 4.
A pressure dressing is applied if required.
Excess Granulation Tissue.
Granulation tissue is a loose collection of fibroblasts, inflammatory cells, and new vessels in an edematous matrix that forms at the base of open wounds. It provides a foundation for reepithelialization. Excessive granulation tissue rises above the wound surface, imposing a barrier to the inward-migrating epidermis. Certain areas, such as the scalp, temples, and lower legs, are prone to form exuberant granulation tissue in open surgical wounds or ulcers. Excess granulation tissue must be removed or suppressed. One technique is to curette the tissue and massage the base with a silver nitrate stick.
Scar Formation.
The evolution of a scar takes several months. New scars are thick and vascular, but gradually, over months, they become less vascular, nonbulky, and flat. Scars that remain thick (hypertrophic scars) or become inappropriately large (keloids) can be treated with intralesional steroids (see Chapter 20 ).
Skin Biopsy
A skin biopsy can be performed simply in the office. Several techniques are practiced, and each has specific advantages ( Table 27.2 ).
| Type of Biopsy | Indications |
|---|---|
| Punch | Most superficial inflammatory and bullous diseases; benign and malignant tumors except malignant melanoma |
| Shave | Superficial benign and malignant tumors (e.g., seborrheic keratoses, warts, dome-shaped nevi, and nonmelanoma malignancies) |
| Excision | Deep inflammatory diseases (e.g., erythema nodosum); malignant melanoma |
Choice of Site.
Generally, biopsies should not be taken from lesions below the knee if other sites are available. Specimens from this area are sometimes difficult for the pathologist to interpret, particularly specimens taken from older patients, in whom mild inflammation and pigmentation produced by stasis may be present. On the face, particularly in the elderly, the arteries are superficial at the following three locations: the temple lateral to the eyebrow (the temporal artery), the nasolabial fold as it intersects the alae (angular artery), and the supraorbital notch at the medial end of the brow (the supraorbital artery). Arteries may be injured by a deep punch biopsy at these sites.
Selection of Lesion for Biopsy.
As a general rule, biopsies should be taken from lesions that are fresh but well-developed. Very early lesions may not have developed diagnostic histologic features, and older lesions may be excoriated or crusted. However, it is important to perform biopsies of very early lesions for diagnosis of vesiculobullous diseases, such as pemphigus and dermatitis herpetiformis. Chronic diseases such as discoid lupus erythematosus may not develop diagnostic features for weeks; biopsies of older lesions should be performed in these cases.
Punch Biopsy
A full thickness of skin can easily be obtained with a cylindrical dermal punch biopsy tool. Disposable punches are very convenient. They are available in 2-, 3-, 3.5-, 4-, 6- and 8-mm widths. The 3-mm punch is adequate for most lesions. Biopsies of the face may be performed with a 2-mm punch to minimize scarring. The resulting wound has smooth, round edges and heals with a slightly depressed scar.
The procedure is adequate for the diagnosis of most tumors. If possible, lesions suspected of being malignant melanoma should be removed completely intact with an excisional biopsy. The quantity of tissue may be inadequate for diagnosis of inflammatory diseases and diseases of adipose tissue, such as erythema nodosum.
Suturing round or oval defects produced by the punch may decrease healing time. Healing by secondary intention is slow but cosmetically acceptable.
Punch Biopsy Technique.
The site is prepared for biopsy with an alcohol pad; a sterile technique is not required. Local anesthesia is induced with 1% lidocaine with epinephrine. Epinephrine is avoided for biopsy near the fingertips. The injection is positioned around and under but not directly into the lesion.
The surrounding tissue is supported by stretching the skin with the thumb and index finger of the free hand. The punch is rotated back and forth between the thumb and forefinger while it is simultaneously pushed vertically into the tissue. Resistance is felt while the instrument penetrates through the dermis but ceases as the punch sinks quickly on entry into the subcutaneous tissue ( Fig. 27.5A–B ).
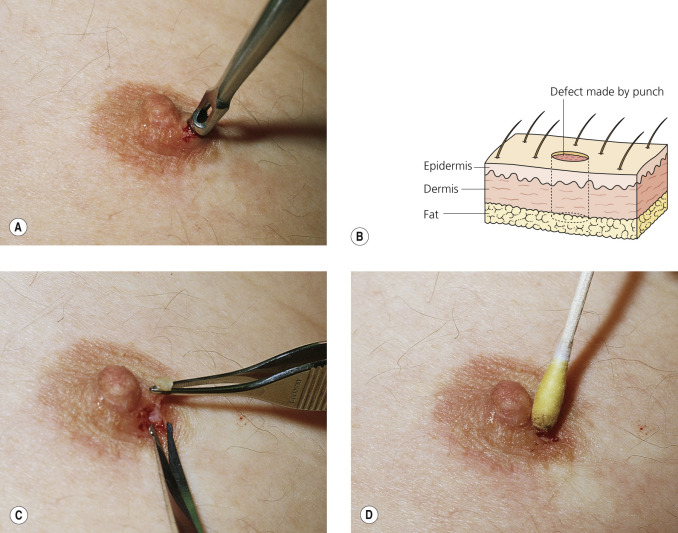
The punch is withdrawn and the cylindrical piece of tissue is gently supported with smooth-tipped forceps; the specimen is cut deep with scissors to include subcutaneous tissue. Forceps with teeth may crush the specimen ( Fig. 27.5C ).
The tissue is immediately transferred to a preservative, and bleeding is controlled with gauze pressure or Monsel’s solution ( Fig. 27.5D ). Some surgeons prefer to apply a single suture to punch defects larger than 3 mm.
Shave Biopsy and Shave Excision
Shave biopsy and shave excision are useful for elevated lesions and when a full thickness of tissue is unimportant. The technique, therefore, is not useful for most inflammatory skin diseases. Shave excision of nevi produces excellent cosmetic results. Any pigmented lesion suspected of being a melanoma should be totally removed by excisional biopsy.
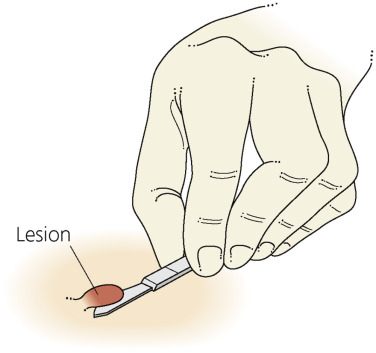
Shave Technique.
The lesion is elevated from the surrounding skin by infiltration with lidocaine. The surrounding skin is supported with the thumb and forefinger of the free hand. The flat surface of a no. 15 surgical blade is laid against the skin next to the lesion. With long strokes, the blade is smoothly drawn through the lesion; back-and-forth sawing motions produce a jagged surface ( Fig. 27.6 ). Several strokes may be required around the periphery of larger lesions. The last attachment of skin may be severed more easily with scissors than with a scalpel blade. Rough edges and contours can be smoothed with electrocautery, and bleeding can be controlled with Monsel’s solution.