(1)
University of Florida, College of Medicine, Gainesville, FL, USA
(2)
Private Practice:, Orlando, FL, USA
6.1 Surgical Anatomy
A. Anatomy of Head and Neck Muscles (Figure 6.1)
Know function of specific muscles and innervation of head/neck muscles (Table 6-1)
Know facial anatomy and important landmarks (Figure 6.2)
Location-specific layers:
Scalp has five layers: epidermis/dermis, subcutaneous tissue, musculoaponeurotic layer, loose subaponeurotic tissue and periosteum
Facial layers (most superficial to deepest): epidermis, dermis, subcutaneous fat, SMAS, muscle, periosteum, bone
Superficial musculoaponeurotic system (SMAS)
Superficial fibromuscular layer enclosing facial muscles of face/neck; extends from frontalis muscle superiorly to platysma muscle inferiorly, temporalis muscle laterally
Allows organized movement of regional muscles during contraction and contributes to appearance of skin tension lines
Protective anatomic plane as sensory nerves and axial blood vessels typically located within or between SMAS and subcutaneous fat; motor nerves usually deep to SMAS
During facelift, SMAS plicated or pulled to draw skin tight
Equivalent of SMAS on scalp is galea aponeurotica, which is a thick inelastic membrane and ideal plane to undermine as it is relatively avascular, separates easily and results in decreased trauma to neurovascular structures
Lip elevators: zygomaticus major/minor, levator labii superioris, levator labii superioris alaeque nasi, levator anguli oris, risorius
Facial expression muscles arise from second branchial archMuscles of mastication arise from first branchial arch
Figure 6.1:
Muscles of the head and neck(Reprint from Nouri, K. Complications in Dermatologic Surgery. Philadelphia, PA: Mosby Elsevier; 2008.)
Figure 6.2:
A: Anatomy/subunits of nose* B: Subunits of the face**C: Anatomy of external ear***Reprint from Nouri, K. Mohs Micrographic Surgery. London, UK: Springer; 2012. **Reprint from Hale E, Karen J, Robins P (eds). Handbook of Dermatologic Surgery. New York, NY:Springer; 2014.
Table 6-1:
Muscles of Head and Neck
Muscle | Function | Innervation |
|---|---|---|
Occipitalis | Pulls scalp posteriorly | Posterior auricular br. of facial nerve (CN VII) |
Frontalis muscle | Elevates eyebrows and wrinkles forehead (horizontal forehead lines) | Temporal br. of CN VII |
Orbicularis oculi | Blinking and tight closure of eyelids (‘crow’s feet’), lesser role as brow depressor (depressor supercilii) | Temporal br. of CN VII (upper portion), zygomatic branch of CN VII (lower portion) |
Corrugator supercilii | Pulls eyebrows medially and downward (vertical glabellar lines) | Temporal br. of CN VII |
Procerus | Pulls medial portion of eyebrows and glabellar skin downward (horizontal glabellar lines over root of nose) | Zygomatic and buccal br. of CN VII per Bolognia, (rare sources say temporal br.) |
Nasalis | Alar flaring and compression (‘bunny lines’ over upper bridge of nose) | Zygomatic and buccal br. of CN VII |
Levator labii superioris | Elevates upper lip | Buccal br. of CN VII |
Levator labii superioris alaeque nasi | Lifts upper lip, dilates nostrils | Buccal br. of CN VII |
Levator anguli oris | Lifts corners of the mouth | Buccal br. of CN VII |
Risorius | Produces smile by drawing back corners of mouth | Marginal mandibular br. of CN VII per Bolognia (other sources say buccal br.) |
Zygomaticus major | Main contributor to smile: elevates and draws corner of mouth laterally | Buccal br. of CN VII |
Zygomaticus minor | Elevates upper lip | Buccal br. of CN VII |
Modiolus | Accounts for cheek dimples in some patients | |
Orbicularis oris | Closes and purses lips (vertical perioral lip lines) | Buccal or marginal mandibular br. of CN VII |
Buccinator | Presses cheek against teeth, allows blowing of cheeks | Buccal br. of CN VII |
Depressor anguli oris | Pulls corner of mouth downward (marionette lines → vertical lines at oral commissure) | Marginal mandibular (MM) br. per Bolognia (most other sources say both MM and buccal br.) |
Depressor labii inferioris | Depresses lower lip | Marginal mandibular br. CN VII |
Mentalis | Protrudes lower lip | Marginal mandibular br. CN VII |
Platysma | Pulls corner of mouth inferiorly, tenses neck (horizontal neck lines) | Marginal mandibular br (upper portion) and cervical br. CN VII |
Table 6-2:
Dissection Planes in Head and Neck
Location | Plane of dissection |
|---|---|
Face | Superficial to SMAS: superficial to mid fat (more superficial in high-risk areas like zygomatic arch, temporal fossa, etc.) |
Nose | Deep to SMAS: superficial to periosteum or perichondrium (below nasalis muscle) |
Scalp | Subgaleal plane: superficial to periosteum (below galea aponeurotica), relatively avascular space |
Trunk/limbs | Deep fat if small excision; just above deep fascia if larger excision |
B. Sensory innervation of Head and Neck (Figure 6.3 and 6.4B, Table 6-3)
Trigeminal nerve provides sensory innervation to facial skin along with motor function to muscles of mastication (masseter, medial/lateral pterygoid, temporalis)
Three main trigeminal divisions: V1 (ophthalmic), V2 (maxillary) and V3 (mandibular)
V1 with five subdivisions: supraorbital (frontal branch), supratrochlear (frontal branch), infratrochlear (nasociliary branch), external nasal (nasociliary branch), and lacrimal nerve
Trigeminal trophic syndrome: injury of CN V (gasserian ganglion), results in dysesthesia often involving nasal ala resulting in sickle-shaped ulceration, treat w/ amitriptyline or carbamazepine
Frey’s syndrome: injury to auriculotemporal branch of CN V in parotid region (carries sympathetic fibers to sweat glands in scalp and parasympathetic fibers to parotid gland), haphazard regeneration leads to redness (vasodilation) and hyperhidrosis of ipsilateral cheek when eating
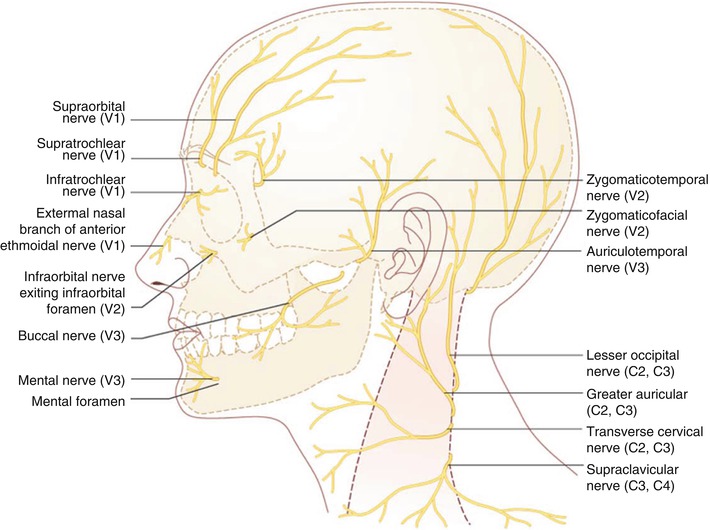
Figure 6.3:
Sensory innervation of head and neck(Reprint from Nouri, K. Complications in Dermatologic Surgery. Philadelphia, PA: Mosby Elsevier; 2008.)
Table 6-3:
Sensory Innervation of Head and Neck
Nerve Branch | Sensory innervation to: | |
|---|---|---|
V1: Ophthalmic branch | ||
Suptratrochlear nerve | Medial forehead, medial upper eyelid, frontal scalp | |
Supraorbital nerve | Most of forehead, portion of frontoparietal scalp, frontal sinus, upper eyelid | |
Lacrimal nerve | Lacrimal gland, conjunctivae, lateral eyelids | |
External nasal branch of anterior ethmoidal (AE) nerve | Nasal dorsum, tip, supratip, and columella CN V→ ophthalmic → nasociliary → AE nerve → external nasal branch Reason why zoster lesions on tip of nose can be sign of eye involvement (since both from nasociliary) | |
Ciliary nerve | Corneal surface CN V→ ophthalmic → nasociliary → ciliary nerve | |
Infratrochlear nerve | Root of nose, upper lateral sidewalls, part of medial canthus, lacrimal sac | |
V2: Maxillary branch | ||
Infraorbital nerve | Medial cheek, upper lip, lower nasal sidewall, nasal ala, lower eyelid | |
Zygomaticofacial (ZMF) nerve | Malar eminence of cheek | |
Zygomaticotemporal (ZMT) nerve | Temple and supratemporal scalp | |
Superior alveolar and palatine nerve | Upper teeth, palate, nasal mucosa and gingiva | |
V3: Mandibular branch (both sensory and motor branches) | ||
Auriculotemporal nerve | Anterior upper half of ear, tragus, preauricular cheek, anterior ½ of meatus, TMJ, external tympanic membrane, temple, temporoparietal scalp | |
Buccal nerve | Cheek, buccal mucosa and gingiva | |
Inferior alveolar | Mandibular teeth | |
Mental nerve | Chin, lower lip | |
Lingual nerve | Anterior 2/3 of tongue (somatic sensation), floor of mouth, lower gingiva | |
Cervical plexus (C2-C4) | ||
Lesser occipital nerve C2 | Neck and postauricular scalp, posterior upper half of ear | |
Greater occipital nerve C2 | Occipital scalp | |
Transverse cervical nerve C2 and C3 | Anterior neck | |
Supraclavicular nerve C3 and C4 | Anterior chest, clavicle and shoulder | |
Greater auricular nerve C2 and C3 | Lateral neck, angle of jaw, inferior lateral cheek, anterior/posterior lower half of ear (include ear lobule), mastoid process, and postauricular skin | |
Other sensory nerves | ||
Facial nerve | CN VII → chorda tympani CN VII → small branches (minor role in sensory) | Taste sensation (anterior 2/3 tongue via chorda tympani), small portion of auditory meatus, concha bowl (variably innervated by branches of vagus and facial nerves), soft palate, pharynx |
Auricular branch of vagus nerve (CN X) | CN X → auricular branch | Posterior ½ of tympanic membrane and posterior wall of external auditory meatus |
Glossopharyngeal (CN IX) | Taste and somatic sensation to posterior 1/3 of tongue | |
Know innervation to following areas:
Great toe web space: deep peroneal nerve
Heel, sole, volar toes: posterior tibial nerve branches (calcaneal and medial/lateral plantar nerves)
Dorsum of foot: superficial peroneal nerve
Lateral malleolus, 5th toe: sural nerve
Lateral sole: sural nerve
Medial malleolus: saphenous nerve
Figure 6.4:
A. Sensory innervation of the lower extremity B. Sensory innervation of the ear(Reprint from Nouri, K. Complications in Dermatologic Surgery. Philadelphia, PA: Mosby Elsevier; 2008.)
C. Motor Innervation of Head and Neck
Mnemonic for CN VII branches: To Zanzibar By Motor Car
Facial nerve exits skull via stylomastoid foramen, enters parotid gland, and then divides into five branches: temporal, zygomatic, buccal, marginal mandibular and cervical
Facial nerve innervates muscles of facial expression (motor) and small component sensory innervation (external auditory meatus, anterior tongue)
All motor nerves innervate respective muscles on muscle’s underside with few exceptions
Three danger zones areas in head/neck for motor nerve injury (Table 6-4)
Nerve | Location | Function | Deficiency |
|---|---|---|---|
Spinal accessory nerve (CN XI) | Nerve courses within posterior triangle of neck in superficial plane, emerges posterior to SCM within 2cm of Erb’s point Erb’s point: midpoint of posterior border of SCM (point where cervical plexus emerges) | Innervates trapezius muscle | Shoulder drooping, winged scapula, inability to abduct arm |
Temporal branch of facial nerve (CN VII) Danger zone between following two lines: ear lobe to lateral edge of eyebrow and tragus to lateral highest forehead crease – nerve most superficial over bony prominence | Nerve courses from a point located 0.5cm inferior to the tragus to a point 2cm superior and lateral to tail of eyebrow before diving beneath frontalis muscle | Innervates frontalis muscle | Inability to raise eyebrow, drooping of ipsilateral eyebrow, inability to close eye completely |
Marginal mandibular branch of facial nerve (CN VII) | Most susceptible to injury anterior to angle of mandible during undermining due to superficial location over bony prominence | Innervates lip depressors | Asymmetry with resultant crooked smile and drooling on affected side |
D. Arterial Supply of Head and Neck (Figure 6.6, Table 6-5)
Vascular supply from external and internal carotid artery
Table 6-5:
Arterial Supply to Head/Neck
External Carotid Artery (ECA) Branches | Internal Carotid Artery (ICA) Branches |
|---|---|
1. Facial artery (terminates by medial canthus) | 1. Ophthalmic artery |
(a) Angular artery | (a) Lacrimal |
(b) Superior labial artery | (b) Supratrochlear (frontal) artery → Axial blood supply for midline forehead flap; success of flap depends on preservation of this artery |
(c) Inferior labial artery | (c) Supraorbital artery |
(d) Lateral nasal artery | (d) Posterior ethmoidal |
2. Superficial temporal artery | (e) Anterior ethmoidal |
(a) Transverse facial artery | (f) Dorsal nasal artery → |
(b) Middle temporal artery | (g) Anterior ciliary artery |
(c) Anterior auricular artery | (h) Central retinal artery |
(d) Frontal branch | |
(e) Parietal branch | |
3. Maxillary artery | |
(a) Infraorbital artery | |
(b) Buccal artery | |
(c) Inferior alveolar artery | |
4. Occipital artery | |
5. Posterior auricular artery | |
6. Lingual artery |
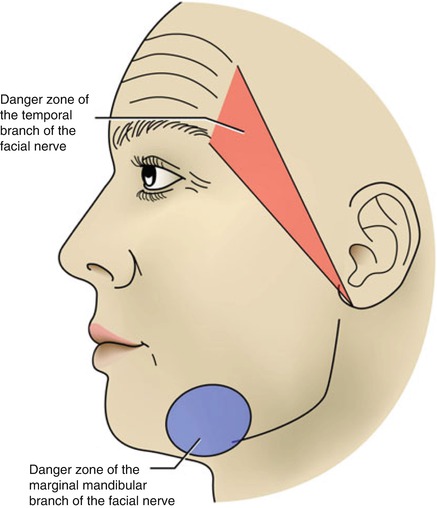
Figure 6.5:
Danger zones of the face(Reprint from Nouri K. Mohs Micrographic Surgery. London, UK: Springer; 2012.)
Of note, facial artery runs superficially across lower border of mandible and then travels toward nose as angular artery
Figure 6.6:
Vascular supply to face(Reprint from Nouri K. Complications in Dermatologic Surgery. Philadelphia, PA: Mosby Elsevier; 2008.)
E. Lymph Nodes of the Head and Neck
Lymph node location | Locations drained by respective lymph nodes |
|---|---|
Postauricular nodes | Upper posterior ear, mastoid, posterior parietal and temporal scalp |
Occipital nodes | Posterior aspect of scalp |
Parotid nodes(includes preauricular and infrauricular nodes) | Upper and lateral face: frontolateral scalp, anterior surface of ears, lower cheeks, forehead, lateral canthal area |
Submental nodes | Central and lower face: central lower lip, chin, floor of mouth, anterior tongue, and chin |
Submandibular nodes | Central and lower face: gingival and mucous membranes, lower eyelids, anterior two thirds of tongue, lips, nose, medial cheeks |
Lymphatic drainage of face in downward diagonal direction.
6.2 Excisions, Flaps, and Grafts
A. Excisions
Basic Excision Principles
Fusiform excision with length typically three times longer than width; sides of wound should be vertical with a flat, even wound base at the level of subcutaneous fat or fascia
Excision should always be made parallel to skin tension lines for best cosmetic result
Skin tension lines: fine wrinkles seen in aged face typically perpendicular to underlying long axis of muscle; lines from tension exerted on skin by facial expression muscles, collagen, and elastic fibers
Variants of elliptical excision can be used in particular locations for a better cosmetic result:
S-plasty or lazy S repair: performed if excision over convex surfaces (ie. jaw, shin, forearm) to ↓ contraction and buckling along length of scar for better cosmetic result
M-plasty: effective for reducing length of scar when it would encroach on important structures (ie. corner of mouth, eyebrow)
Crescent excision: results in shorter curvilinear scar and can be oriented along curved skin tension lines or cosmetic subunit junction lines (ie. cheek, chin)
Of note, lesions on the lip with a size equal or less to 1/3 the length of lower lip can be repaired with primary closure after wedge excision due to laxity of the lip
Cosmetic subunits
Major structural areas of face separated by contour lines or boundaries
Units arranged by similarity in topographic anatomy, texture, pigmentation, amount of sun exposure, sebaceous gland and hair type/density
Major units: forehead, temples, eyelids, nose, cheeks, upper and lower lips, chin and ears
Units within nose: dorsum, nasal sidewall, soft triangle, tip, alar lobule, columella
Contour lines between cosmetic units is an ideal place to hide surgical scars (i.e., hairline, alar or nasolabial crease, eyebrows, philtrum, vermilion cutaneous interface)
Defects should be repaired with tissue from within the same cosmetic unit to preserve consistency and for best cosmetic outcome
Wounds may contract as fast as 0.75 mm/day
Wound Healing
Primary vs. secondary intention healing
Primary intention: direct closure of wound by approximating wound edges together (side to side closure, flaps, grafts)
Secondary intention: wound left open and allowed to heal from inner to outer surface
Wound contraction (maximal at 2 months after re-epithelialization)
Concave skin wounds (ie. inner ear, nasal alar crease, temple, conchal bowl) heal with best with secondary intention (vs. primary)
Convex surfaces (ie. malar cheek, vermilion border of lip, tip of nose) not optimal for healing by secondary intention and may cause ectropion or eclabion in areas with free margin of skin (nose, eyelids)
Wound healing: Four sequential overlapping stages
Vascular phase: thrombin/exposed collagen results in stimulation of platelets, which release PDGF and other factors important for angiogenesis and fibroplasia → platelets aggregate forming hemostatic plug and damaged vessels are pressed together causing adherence to one another → overall result is hemostasis
Inflammatory phase: neutrophils (first cell to arrive, often within first hour after injury) and macrophages (most important cell in healing process) recruited to wound site, phagocytosis of debris/bacteria
Proliferative phase: re-epithelialization within first 24 h of injury, production of collagen (type III); macrophages release fibronectin (which attracts fibroblasts) and other factors which induce angiogenesis and granulation tissue formation
Wound contraction and remodeling: contraction via myofibroblasts, maximum strength of scar reached is 70-80% of original strength prior to injury
Table 6-6:
Types of Superficial Repair
Repair | Pros | Cons | Use for: |
|---|---|---|---|
Simple interrupted | + provides wound eversion + allows high-low correction + individual sutures removed without disturbing remaining | − ↑ overall closure time − ↑ net suture bulk with more prominent suture marks, skin irritation | |
Running | + ↓ closure time + suture bulk spread over entire wound | − integrity depends solely on knots on either end | Use with minimal tension wounds |
Vertical mattress | + relieves tension + wound eversion | − tendency to leave permanent suture marks | High tension areas |
Horizontal mattress | + ↑ holding tension + wound eversion + hemostasis | − ↑ tissue ischemia − railroad track marks | Tight situation where vertical mattress not possible |
Running subcuticular | + avoids any suture marks along skin surface | − ↑ reactivity − ↑ overall closure time | Minimal tension and mobility |
Scar strength: 5% at 2 weeks 15% at 3 weeks 40% at 6 weeks 80% at 1 year
Best with polypropylene glycol due to ↓ tissue reactivity
B. Flaps
May be classified based on:
Blood Supply
Axial pattern flap-relies on specific artery for blood supply
Random pattern flap
Primary Motion
Advancement
Rotation
Transposition
Flaps can redirect wound tension vector and recruit tissue laxity from adjacent skin
Be able to identify type of flap based on outline of scar (Table 6-7)
C. Grafts
Skin completely detached from donor site; full-thickness, split-thickness and composite
Full-Thickness Skin Graft (FTSG)
Epidermis + full thickness dermis
Advantages: better overall cosmesis (compared to STSG), less wound contracture, retention of appendages
Disadvantages: increased metabolic demand (due to increased thickness) thus size of FTSG limited, increased rate of graft failure since more vulnerable to necrosis
Donor sites: preauricular, postauricular, conchal bowl, nasolabial, supraclavicular, inner arm
Typically FTSGs placed over convex and concave sites (ie. medial canthus, helix, nasal tip, and nasal ala); must remove fat as this may compromise viability of graft
Graft should be 10-20% larger than defect size to prevent undersized graft and account for graft contracture (typically up to 15% contraction)
One week postop: violaceous appearance (resist debridement even if black and potentially necrotic) → monitor site for another week as even if necrotic, can serve as biologic dressing
Two weeks postop: often changes from a violaceous to pink color
Table 6-7:
Types of Flaps: Advancement, Rotation and Transpositional
Type of Flap | Description | Appearance |
|---|---|---|
Advancement Flap Unidirectional, uncomplicated advancement of leading edge of flap | ||
Unilateral advancement flap (U-plasty) | Defect excised as square and incision extended in same direction on two but opposite parallel sides of defect; burow’s triangle created at end of each extension and flap slides over defect creating U-shaped scar |  |
Bilateral advancement flap (H-plasty) | Double U-plasty or double advancement flap; two U-plasty flaps created as mirror images of one another; most useful for scalp and eyebrow defects (H-plasty) |  |
Bilateral T-plasty (A-T, O-T) | Linear repair of wound perpendicular to pre-existing cosmetic boundary; useful for above brow, upper cutaneous lateral lip |  |
Burow’s advancement flap | Defect excised in shape of equilateral triangle and one arm of triangle extended; burow’s triangle created at contralateral side of extension and tissue slides to cover defect |  |
Island pedicle flap | Special advancement flap: most of vascular supply from a subcutaneous pedicle (remains attached to central portion of flap) and all dermal margins of flap severed before advanced |  |
Rotation flap Recruits adjacent tissue laxity and directs wound tension vectors away from primary surgical defect; curvilinear incision (arc) adjacent to primary defect and flap rotated to primary defect site; useful for scalp, temple, and medial cheek defects | ||
Dorsal nasal rotation flap | Special type of rotation flap; long sweeping arc that involves rotation of entire nasal dorsum (elevated at level of perichondrium or periosteum) |  |
Bilateral advancement rotational flap (O – Z flap) | Bilateral rotation flap converting circular defect into a Z-shaped incision line, most useful on scalp (can be purely rotational or advancement with rotation) |  |
Transposition Flap Most complex design, redirects wound closure tension, moves tissue from area of surplus to area of need by transpositioning across intervening islands of unaffected tissue | ||
Rhomboid transposition flap | Rhomboidal-shaped flap created adjacent to round or oval defect and transposed into defect |  |
Bilobed transposition flap | Recruits tissue from proximal nasal dorsum (more laxity) and transfers to defect, useful on distal nose |  |
Nasolabial transposition flap | Flap from medial cheek adjacent to melolabial fold transposed to alar wound, useful in lateral and central alar wounds |  |
Z-plasty | Useful for scars crossing relaxed tension lines or releasing contractures (redistributes tension over wound) |  |
Paramedian forehead flap | 2 stage flap for repair of subtotal to total nasal defects; forehead flap designed vertically to preserve supratrochlear artery supply; flap rotated 180 degrees and sewn into nasal defect; 2-3 weeks later pedicle divided and repositioned | Axial pattern flap as well |
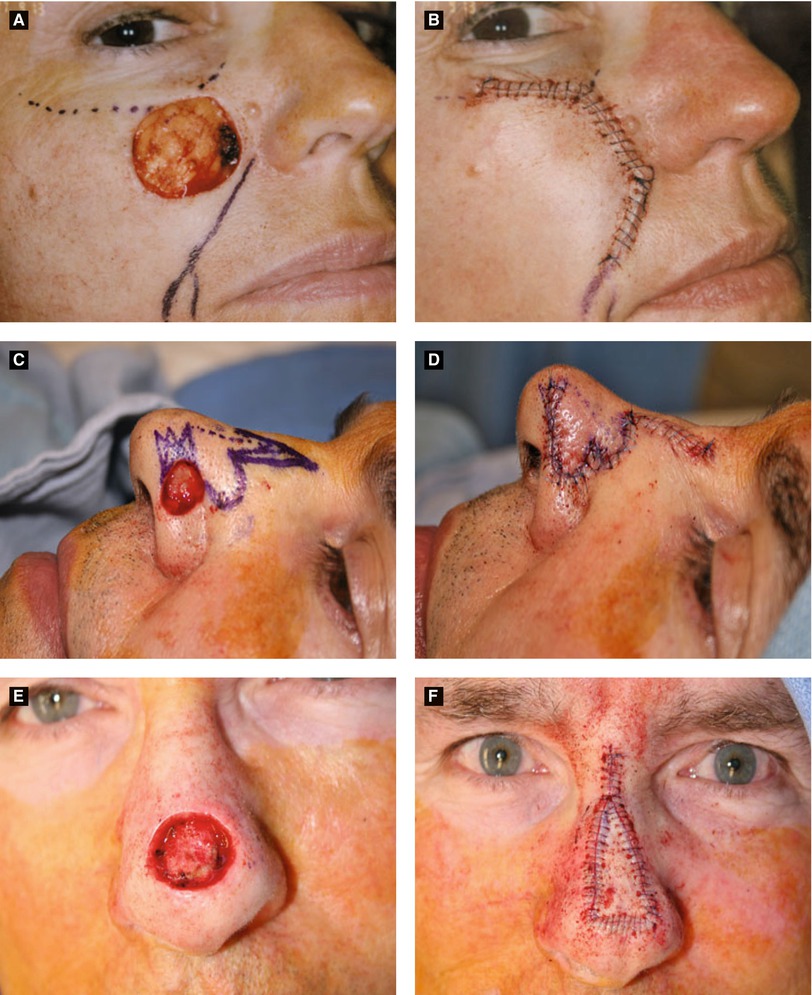
Figure 6.7:
A: Advancement flap* B: Advancement flap*C: Bilobed flap* D: Bilobed flap*E: Island pedicle flap* F: Island pedicle flap**Reprint from Nouri, K. Mohs Micrographic Surgery. London, UK: Springer; 2012.
Thin STSG: 0.005 to 0.012 in
Medium STSG: 0.012 to 0.018 in
Thick STSG: 0.018 to 0.030 in
Split-Thickness Skin Graft (STSG)
Epidermis + partial thickness dermis
Advantages: ability to cover large defects (especially if graft fenestrated), higher likelihood of survival as less metabolic demand, allows for detection of tumor recurrence in cutaneous oncology
Disadvantages: less cosmetically desirable color and texture, granulation tissue at donor site, increased contracture at wound site (more than with FTSG), lack adnexal structures (do not produce sebum, hair, sweat)
Donor sites: buttocks, thighs, arms, abdomen
1 week postop: pink to skin-colored
Composite Graft
Epidermis + dermis + one more component (typically cartilage)
Advantages: ability to restore missing cartilage in primary defect, maintains proper tissue architecture and function
Disadvantages: highest metabolic demand (thus, highest likelihood of failure), size limited (due to blood supply)
Donor sites: helix of ear, conchal bowl
Most commonly used in nose (commonly nasal ala → cartilage restores proper function and prevents alar collapse during inspiration) and donor site typically crus of helix of ear
Stages of Graft Survival (Table 6-8)
Skin graft must re-establish blood supply at recipient sites
Three stages: imbibition, inosculation, neovascularization
Table 6-8:
Stages of Skin Graft Survival
Stages | Description |
|---|---|
1. Imbibition | First 24-48 hours (ischemic period) |
Graft sustained by plasma exudate from wound bed | |
Fibrin attaches graft to new bed | |
Graft becomes edematous, ↑ weight by up to 40% | |
2. Inosculation | Begins 48-72 hours, lasts up to 7-10 days (graft vessels anastomose) |
Revascularization linking dermal vessels in graft to recipient bed | |
Rationale for delayed grafting over sites devoid of perichondrium or periosteum (allows formation of granulation tissue with ↑ survival rate) | |
3. Neovascularization | Occurs temporally with inosculation |
Capillary ingrowth from recipient wound base and sidewalls to graft | |
If optimal conditions, full circulation reestablished within 4-7 days | |
4. Maturation | Occurs months later Reinnervation of graft typically within 2 months of graft but may not be complete for months to years (full sensation may never fully return) |
6.3 Surgical Complications
Hematoma
Risk of bleeding greatest in first 48 hours (especially in immediate posotoperative period)
Provides medium for bacteria, prevents wound healing, ↑ wound tension (± dehiscence)
Two types of hematoma: stable and expanding
Stable hematoma
Non-expanding ecchymotic firm to fluctuant mass with sensation of pressure
Small, stable, non-infected and not compromising tissue viability → no surgical intervention necessary (observation w/ warm compresses to hasten resorption)
Expanding hematoma
Enlarging ecchymotic fluctuant to firm mass with new onset pain (often throbbing)
Medical emergency if expanding hematoma in periorbital and cervical locations
If very early hematoma (warm, swollen, fluctuant) → intervention recommended to prevent further progression (same intervention as for expanding hematoma)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree