(1)
University of Florida, College of Medicine, Gainesville, FL, USA
(2)
Private Practice:, Orlando, FL, USA
1.1 Embryology
Table 1-1:
Development of Cutaneous Structures
Gestational Age (Estimated) | Epidermal Development | Hair, Nail and Gland Development | Dermal/Subcutaneous Development | |
|---|---|---|---|---|
1st trimester | ~3–4 weeks | Single layer of ectoderm | Germinal layer produces entire epidermis | |
~6 weeks | Outer flattened periderm and inner, cuboidal germinal (basal) layer | Germinal layer in contact w/ underlying mesenchyme | ||
~7 weeks | Fetal basement membrane | Tooth primordia | ||
~8–12 weeks | Epidermal stratification begins ~8 weeks Appearance of → Melanocytes → Langerhans cells → Merkel cells | Completed by 2nd trimester | Dermal-subcutaneous boundary distinct | |
~9–12 weeks | Appearance of anchoring filaments/hemidesmosomes | Hair follicle and nail primordia seen | ||
2nd trimester | ~12 weeks | Formation of dermo-epidermal junction (DEJ) | Nail bed starts to keratinize, proximal nail fold forms | Type III collagen appears |
~12–14 weeks | Parallel ectodermal ridges (fingerprints) | Eccrine and sebaceous gland primordia seen | Fibroblasts actively synthesizing collagen and elastin in dermis | |
~12–24 weeks | Melanin production (12–16 wks), melanosome transfer (20 wks) | Hair follicles differentiate during 2nd trimester (7 concentric layers present) | ||
~15–20 weeks | Periderm is shed (periderm is part of vernix caseosa) [20–21 weeks] | Follicular keratinization, nail plate completely covers nail bed | Papillary/reticular boundary distinct, dermal ridges appear | |
~22 weeks | Trunk eccrine gland primordia | Elastic fiber seen | ||
~22–24 weeks | Mature epidermis complete (w/ interfollicular keratinization) | Adipocytes appear under dermis |
1.2 Epidermis
Functions as a mechanical and antimicrobial barrier; protects against water loss and provides immunological protection; thickness varies from 0.04 mm (eyelid skin) to 1.5 mm (palmoplantar skin)
Divided into four layers (each with characteristic cell shape and intracellular proteins): stratum corneum, stratum granulosum, stratum spinosum, and stratum basale (germinativum); of note, stratum lucidum is additional layer in palmoplantar skin
Keratinocytes
Ectodermal derivation; keratinocytes comprise approximately 80–85% of epidermal cells
Total epidermal turnover time: average 45–60 days (30–50 days from stratum basale to stratum corneum and approximately 14 days from stratum corneum to desquamation)
Epidermal self-renewal maintained via stem cells in basal layer of interfollicular epithelium and the bulge region of hair follicles (latter location only activated with epidermal injury)
Keratinocytes produce keratin filaments (syn: intermediate filaments or tonofilaments), which form the cell’s cytoskeletal network; this provides resilience, structural integrity, along with serving as a marker for differentiation (ie. basal layer: K5/14)
Six different types of keratin filaments: type I/II are epithelial/hair keratins, type III-VI include desmin, vimentin, neurofilaments, nuclear lamins, and nestin
>50 different epithelial/hair keratins, expressed as either type I (acidic) or type II (basic), and type I/II coexpressed together as a heterodimer (i.e., K5/14)
Type I (acidic) epithelial keratins: K9–28, chromosome 17
Type I (acidic) hair keratins: K31–40 (old nomenclature: hHa1–hHa8, Ka35, Ka36)
Type II (basic) epithelial keratins: K1–8 and K71–80, chromosome 12
Type II (basic) hair keratins: K81–86 (old nomenclature: hHb1–hHb6)
Table 1-2:
Keratin Filament Expression Pattern
Type II | Type I | Location of expression | Associated diseases |
|---|---|---|---|
1 | 10 | Suprabasal keratinocytes | Epidermolytic hyperkeratosis, Unna-Thost PPK |
1 | 9 | Palmoplantar suprabasal keratinocytes | Vorner PPK |
2 (2e) | 10 | Granular and upper spinous layer | Ichthyosis bullosa of Siemens |
3 | 12 | Cornea | Meesman corneal dystrophy |
4 | 13 | Mucosal epithelium | White sponge nevus |
5 | 14 | Basal keratinocytes | Dowling-Degos disease, EBS |
6a | 16 | Outer root sheath | Pachyonychia congenita I |
6b | 17 | Nail bed | Pachyonychia congenita II |
8 | 18 | Simple epithelium | Cryptogenic cirrhosis |
K81 K86 | Hair | Monilethrix | |
19 | Stem cells |
Of note, second cytoskeletal network formed by actin filaments
Do not confuse Dowling-Degos with Degos disease:Dowling-Degos: AD, reticulated pigmentation over skin foldsDegos (malignant atrophic papulosis): occlusion + tissue infarction
Stratum Basale (Germinativum)
Basal layer just above basement membrane; contains keratinocytes, melanocytes, merkel cells and Langerhans cells (latter mainly in stratum spinosum)
10% of cells in basal layer are stem cells
Expression of ornithine decarboxylase (ODC), which is a marker for proliferative activity
(ODC stimulated by UVB and partially blocked by retinoic acid/corticosteroid/vitamin D3)
De novo expression of K5/14 occurs, forming keratin filaments which insert into both desmosomes and hemidesmosomes and form keratinocyte cytoskeleton
Hemidesmosomes allow attachment of basal keratinocyte to basement membrane
Flegel’s disease, Harlequin ichthyosis: ↓ lamellar granules (LG)X-linked ichthyosis: absent steroid sulfatase in LG.Congenital ichthyosiform erythroderma: ↑ LG but structurally abnormal
Stratum Spinosum
Polyhedral-shaped cells with round nucleus and ‘spiny’ appearance on H&E (due to desmosomal attachments between cells); layer contains keratinocytes and Langerhans cells
New synthesis of K1/K10; K5/14 still present (not de novo)
Cells contain lamellar granules (syn: lamellated bodies or odland bodies): intracellular lipid-carrying granules formed w/in Golgi in upper spinous layer; contain glycoproteins and lipid precursors which are discharged into intercellular space between granular and cornified layer; forms lamellar sheets (ceramide) or ‘mortar’ which acts as intercellular cement for corneocytes (‘bricks’), thus contributing to formation of cutaneous lipid barrier
Types of cell junctions prominently seen in this layer and in granular layer (Figure 1.1):
Desmosomes: calcium-dependent cell-cell adhesion molecules between keratinocytes; serve as attachment sites for cytoskeleton (intermediate filaments); each desmosome made up of several proteins:
Transmembrane proteins: desmoglein 1/3, desmocollin 1/2 (desmosomal cadherins)
Desmosomal plaque proteins: plakoglobin (γ-catenin), desmoplakin 1/2, keratocalmin, desmoyokin, band 6 protein, envoplakin
Adherens junctions (zonula adherens): transmembrane classical cadherins (namely E and P) linked to actin cytoskeleton via cytoplasmic plaque proteins (α, β, γ-catenin)
Tight junctions (zonula occludens): seal intercellular space, prevent diffusion of solutes between cells and maintain cell polarity; major constituents are claudins and occludins
Gap junctions: transmembrane channels formed by six connexin monomers, allows for cytoplasmic continuity and communication between cells
Know particular diseases associated with defects or antibodies against certain cell junction proteins (Figure 1.1)
Figure 1.1:
Skin diseases associated with cell junctions
Plakoglobin: only common protein between adherens junction and desmosome
Ichthyosis vulgaris: ↓ profilaggrin, ↓ KHGLamellar ichthyosis: ↑ profilaggrin, ↑ granular cell layerPsoriasis: ↑ involucrin, ↓ loricrin, ↑ K6/16
Stratum Granulosum
Cells with more flattened appearance; contain dense keratohyalin granules
Granular cells start to lose their nuclei but retain dense keratin filaments
Expression of K2 (modified from K1) and K11 (modified from K10)
Keratohyalin granules (KHG): dense stellate globules which contain profilaggrin, loricrin, and involucrin (latter two function in cornified cell envelope)
Filaggrin: keratin filament aggregating protein in KHG; binds intermediate filaments and organizes into fibrils; initially cleaved from profilaggrin (when granular layer transformed into cornified layer) and is degraded into free amino acids
Cornified cell envelope [CE] (Figure 1.2): highly cross-linked lipid-rich flexible structure enveloping corneocytes; serves as insoluble exoskeleton and rigid scaffold for internal keratin filaments; provides both mechanical and water permeability barrier
CE assembly begins in granular layer where several proteins cross-linked by transglutaminase into γ-glutamyl lysine isopeptide bonds → rendering CE insoluble
CE comprised of lipid layer and several covalently cross-linked proteins: involucrin, loricrin, filaggrin, small proline-rich proteins (SPRs), envoplakin, and serine proteinase inhibitor called skin-derived anti-leukoproteinase (SKALP)
Loricrin: major protein component of CE, appears in granular layer within KHG along with profilaggrin, cross-links with involucrin
Involucrin: substrate for transglutaminase cross-linking in granular layer; forms insoluble cell boundary; early differentiation marker and upregulated in psoriasis
Figure 1.2:
Cornified envelope (CE)
Stratum Corneum
Provides mechanical protection, impermeability and barrier to water loss
Brick and mortar model: lipid-depleted, protein-rich corneocytes (‘bricks’) surrounded by extracellular lipid-rich matrix (‘mortar’)
Corneocytes composed of high weight keratins embedded in filaggrin-rich matrix
Urocanic acid (UCA): filaggrin degradation product found naturally in the cornified layer; absorbs/blocks UV radiation and forms natural moisturization factor (NMF) with other filaggrin degradation products (amino acids, pyrrolidone carboxylic acid); NMF allows stratum corneum to remain hydrated even in drying conditions
Ceramide is a major lipid barrier of skin; other barrier lipids include cholesterol, cholesterol sulfate, and fatty acids
Of note, steroid sulfatase cleaves cholesterol sulfate to cholesterol; enzyme abnormal in X-linked ichthyosis
1.3 Basement Membrane Zone (BMZ)
Selective barrier between the epidermis and dermis; allows for interaction between the two areas and provides anchoring of epidermis to dermis
Skin has 2 main BMZs: dermo-epidermal junction (major BMZ) (Figure 1.3) and dermal blood vessels
Figure 1.3:
Dermo-epidermal junction zone (DEJ)
Contains 4 distinct zones on electron microscopy (EM): inferior portion of basal keratinocyte, lamina lucida, lamina densa and sublamina densa
Be able to identify BMZ components on electron microscopy (EM) (Figure 9.7A)
Table 1-3:
Macromolecules in BMZ
Layer of BMZ | Structure | Associated Macromolecules |
|---|---|---|
Basal keratinocyte/Plasma membrane | Hemidesmosome | BPAG1 (230kDa), BPAG2 (180kDa), α6β4 integrin, plectin |
Lamina lucida | Anchoring filaments | Laminin, portion of BPAG2 |
Lamina densa | Anchoring plaque | Type IV collagen, laminins, heparan sulfate |
Sublamina densa | Anchoring fibril | Type VII collagen, fibrillin, anchoring plaque (type IV collagen), type I and III collagen |
A. Inferior Portion of Basal Keratinocyte
Hemidesmosome (HD)
Appears as thickened area interspersed along plasma membrane of basal keratinocyte; provides attachment between basal keratinocyte and extracellular matrix
Composed of following macromolecules: BPAG1, BPAG2, integrin, and plectin
Tonofilaments (or keratin filaments) insert into hemidesmosomes
BPAG1 (230 kDa)
Intracellular glycoprotein in plakin family which is associated with the cytoplasmic plaque domain of hemidesmosomes; promotes adhesion of intermediate filaments with plasma membrane (likely binds or anchors filaments to HD)
BPAG2 (180kDa, Collagen XVII)
Transmembrane (mainly extracellular) protein belonging to collagen family; interacts with BPAG1, β4 integrin, and plectin
Divisions of protein: amino terminus (intracellular), transmembrane portion, extracellular carboxy terminus (in lamina lucida); most antibodies in bullous disorders target extracellular domain (proximal NC16A and distal carboxy terminus)
NC16A domain (1st extracellular segment): typically targeted by bullous pemphigoid (BP), pemphigus gestationis, linear IgA bullous dermatosis (LABD)
Carboxy terminus (C-terminal): cicatricial pemphigoid (CP) tends to target this portion
Three target antigens seen in CP: BPAG2, laminin-5 (epiligrin), α6β4 integrin
Integrin
Transmembrane cell receptor consisting of two subunits (α and β); located at basal layer of epidermis and promotes both cell-cell and cell-matrix interactions
α6β4: hemidesmosome-associated integrin; binds intermediate filaments intracellularly, laminin-5 (now called laminin-332) in lamina lucida, and HD proteins (plectin, BPAG2)
Autoantibody to β4 → CP (ocular); β4 mutation → JEB with pyloric atresia
Plectin
Intracellular protein belonging to plakin family; associated with cytoplasmic plaque domain of hemidesmosome; links intermediate filaments to plasma membrane and cross-links HD proteins
Plectin mutation → EBS w/ muscular dystrophy
B. Lamina Lucida
Electron-lucent zone under hemidesmosome on EM; weakest link of BMZ
Comprised of anchoring filaments (laminin-332), laminin-1, fibronectin, nidogen (entactin), uncein and portion of BPAG2
Anchoring Filaments
Delicate filaments emanating perpendicularly from HD which stretch from plasma membrane to lamina densa; product of basal keratinocytes; smaller than anchoring fibrils
Laminin-332: also known epiligrin (truncated laminin), laminin-5, kalinin, and nicein; glycoprotein serving as major component of anchoring filaments; major attachment factor for keratinocytes and binds α6β4 integrin at hemidesmosome
C. Lamina Densa
Electron-dense zone below lamina lucida appearing as dense line with closely stippled dots on EM
Type IV collagen: major component and characteristic collagen of BMZ; highly cross-linked sheet-like pattern provides flexibility to basement membrane
Additional components: laminins, entactin (nidogen-1), and heparan sulfate (negatively-charged hydrophilic proteoglycan which provides selective permeability barrier)
D. Sublamina Densa
Contains anchoring fibrils, anchoring plaques, elastic microfibrils (without elastin), and linkin
Anchoring Fibril
Primary constituent is type VII collagen; appears larger than anchoring filaments and emanates perpendicularly down from lamina densa into papillary dermis
Connects lamina densa to anchoring plaques (type IV collagen) in dermal matrix
Intercalation with banded collagen fibrils of papillary dermis: forms fan-shaped clumps
Type VII collagen autoantibodies in both EB acquisita (EBA) and bullous SLE; type VII mutation in dystrophic EB (DEB)
Anchoring Plaque
Primary component is type IV collagen; site where anchoring fibrils attach from above and fibrillar collagen (type I and III) attach from below; electron-dense oval structures seen under lamina densa on EM
Table 1-4:
Diseases Associated with Epidermal/Dermal Proteins
Protein | Associated Disease |
|---|---|
Plectin | EBS with muscular dystrophy, paraneoplastic pemphigus (PNP) |
α6β4 integrin | JEB with pyloric atresia, cicatricial pemphigoid (CP) – ocular |
BPAG1 | Bullous pemphigoid (BP), PNP |
BPAG2 | NC16A → BP, linear IgA bullous dermatosis (LABD), pemphigoid gestationis Carboxy terminus → CP |
Laminin-332 (5) | JEB (Herlitz), CP (↑ risk of cancer) |
Type VII collagen | Dystrophic EB (mutated), EBA, bullous SLE |
Plakoglobin | Naxos disease |
Desmocollin 1 | Subcorneal pustular dermatosis (type of IgA pemphigus) |
Desmoglein 1 | Striate PPK, pemphigus foliaceous, pemphigus vulgaris (mucocutaneous), bullous impetigo, staphylococcal scalded skin syndrome (SSSS), PNP |
Desmoglein 3 | Pemphigus vulgaris (mucosal-dominant and mucocutaneous), PNP |
Desmoglein 4 | Monilethrix (autosomal recessive) |
Desmoplakin 1/2 | Carvajal syndrome, striate PPK, skin fragility/woolly hair syndrome, PNP |
Plakophilin | Ectodermal dysplasia/skin fragility syndrome |
Connexin 26 | KID syndrome, Vohwinkel syndrome, PPK with deafness |
Connexin 30 | Hidrotic ectodermal dysplasia (HED) |
Connexin 30.3/31 | Erythrokeratoderma variabilis (EKV) |
β-catenin | Pilomatricoma (multiple may be associated with myotonic dystrophy) |
Loricrin | Vohwinkel (variant), progressive symmetric erythrokeratoderma |
Filaggrin/KHG | Atopic dermatitis, ichthyosis vulgaris |
Transglutaminase | TG3 → dermatitis herpetiformis, TG1 → lamellar ichthyosis |
1.4 Melanocytes, Langerhans, and Merkel Cells
Melanocyte
Pigment-producing dendritic cell derived from neural crest; found in skin, hair, uveal tract of eye (choroid, iris, ciliary body), leptomeninges, and inner ear (striae vascularis of cochlea)
Survival/migration during embryogenesis depends on specific interactions such as c-kit activation contributing to migration and development of melanocytes and melanoblasts
Resides in basal layer with ratio of 1 melanocyte to 10 basal keratinocytes (do not confuse with epidermal melanin unit where 1 melanocyte in contact with 36 keratinocytes)
Melanocytes do not form junctions with keratinocytes (hence, artifactual halo on H&E)
Function: production of melanin pigment with subsequent transfer to keratinocytes, absorption of UV radiation and protection from UV-induced mutations
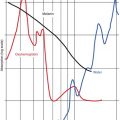
Melanin: synthesized in melanosome (specialized type of lysosome) and passes through series of stages (I to IV) before melanosome transferred to keratinocyte via phagocytosis of melanocyte tips (apocopation); melanin precursors acted upon by copper-dependent enzyme tyrosinase; two types of pigment (Figure 1.4):
Pheomelanin: red-yellow in color, synthesized in pheomelanosomes (spherical structure, microvesicular internal structure)
Eumelanin: brown or black in color, eumelanosome (oval-shaped, longitudinally oriented with lamellar internal structure)

Figure 1.4:
Melanin biosynthetic pathway
Melanin stimulated by melanocyte-stimulating hormone (MSH), which is derived from larger precursor propiomelanocortin (POMC); POMC also a precursor for ACTH, which is why ↑ hyperpigmentation seen in Addison’s disease
Melanocortin-1 receptor (MC1R) controls which type of melanin is produced by melanocytes; loss of function in MC1R results in ↑ pheomelanin (red hair) and ↓ eumelanin; thus, fair skin without the more protective pigment and more prone to damage from UV radiation with subsequent ↑ risk for melanoma
Hair melanocytes: one melanocyte to 5 keratinocytes; graying caused by gradual decrease in number of follicular melanocytes
Chronic sun exposure results in melanocytes creating larger melanosomes
Racial differences NOT due to differences in number of melanocytes, but rather the size, distribution and number of melanosomes (all races have SAME melanocyte density)
Dark-skinned: larger melanosomes, ↑ melanization, ↓ melanosome degradation, and melanosomes transferred as individual organelles
Light-skinned: smaller melanosomes and transferred as membrane-bound clusters (with 3–6 melanosomes)
Be able to identify EM image of Langerhans cell (Figure 9.7B)
Langerhans Cell (LC)
Bone marrow-derived dendritic cell with monocyte-macrophage lineage found in stratum spinosum; constitutes 3–5% of cells of epidermis; contains actin and vimentin
Critical in recognizing and presenting foreign antigens to specific T lymphocytes
Connected to keratinocytes via E-cadherin receptors
On EM, Langerhans cell with folded nucleus and distinct intracytoplasmic organelles (Birbeck granules: striated appearance with either rod-shape and/or tennis-racquet-shape)
Exposure to UV radiation causes depletion of LCs and decreases ability to present antigen
Langerhans cell histiocytosis:Letterer-Siwe – acute disseminatedEosinophilic granuloma – bone (cranium)Hand-Schuller-Christian – diabetes insipidus, exophthalmos, bone lesionsHashimoto-Pritzker – self-healing
Merkel Cell
Ectoderm-derived cell (less likely neural crest-derived) functioning as mechanoreceptor (slow adapting, type I); found among basal keratinocytes
Found in areas with high tactile sensitivity (lips, fingers, ORS of hair follicle, oral mucosa)
EM shows microvilli at cell surface with dense core granules, lobulated nucleus, and intermediate filaments assuming whorled arrangement near nucleus (dot-like pattern)
Markers: cytokeratin (CK) 20 (specific for merkel cells in skin), also contain CK8, 18, and 19
Contain battery of neuropeptides and neurotransmitter-like substances:
Neuron-specific enolase (NSE), vasoactive intestinal peptide (VIP), calcitonin gene-related peptide (CGRP), chromogranin A, synaptophysin, and met-enkephalin
Know neuropeptides found within merkel cells
1.5 Dermis
Mesoderm-derived components
Divided into superficial papillary dermis and deep reticular dermis (latter with larger collagen bundles and mature branching elastic fibers)
Collagen
Family of fibrous proteins, 20+ genetically distinct types identified; provides structural stability and accounts for 70–80% dry weight of dermis; major dermal constituent
Composed of 3 chains combined into a triple helix configuration; contains Gly-x-y repeats (glycine always 3rd residue, x frequently proline, y often hydroxylysine or hydroxyproline)
Glycine is most abundant amino acid in collagen
Collagen degraded by interstitial collagenases (metalloproteinases or MMPs)
Collagen synthesis stimulated by: retinoic acid
Collagen synthesis inhibited by: IL-1 (↑ MMP expression), glucocorticoids, IFNγ, TNFα, D-penicillamine, UV irradiation
Table 1-5:
Types of Collagen
Collagen | Location | Associated Diseases |
|---|---|---|
I | Dermis, bone, ligament/tendon | Ehers-Danlos syndrome, arthrochalasia (EDS type VII), osteogenesis imperfecta |
II | Vitreous humor, cartilage | |
III | Fetal skin, blood vessels | EDS vascular (type IV) |
IV | Basement membrane | Alport and Goodpasture syndrome
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|