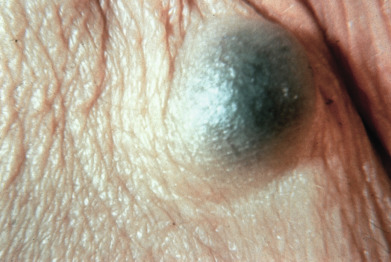
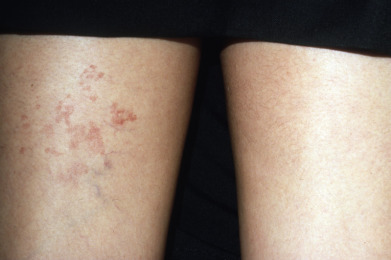
Vascular tumors range from red to blue, depending on the degree of vascular stasis and deoxygenation of hemoglobin. When associated with thrombosis or consumptive coagulopathy, the lesions often become hard and tender. The clinician should attempt to distinguish vascular proliferative lesions from vascular malformations, as the former tend to respond to beta blockers, whereas the latter do not. Malformations include nevus flammeus, salmon patch, nevus anemicus, and cutis marmorata telangiectatica congenita. Some vascular malformations are associated with overgrowth of surrounding tissues and can lead to considerable morbidity. This portion of the atlas will focus on the clinical findings of dermal tumors, including fibrous and vascular proliferations, as well as growths, in addition to those composed of muscles, nerves, and fatty tissue.
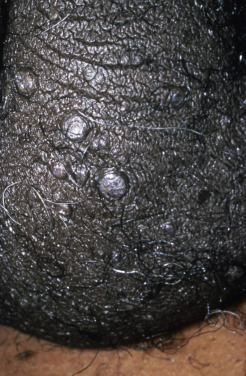
A biopsy may be required for the definitive diagnosis of dermal neoplasms, but the color, morphology, and distribution of the lesions can often lead to an accurate clinical diagnosis. Dermatofibromas present as firm, pink-to brown dermal nodules with overlying epidermal acanthosis imparting a dull or velvety appearance to the skin. A characteristic dimpling sign occurs when the surrounding skin is compressed laterally. Granular cell tumors tend to be larger, but are accompanied by a similar velvety or verrucous appearance of the overlying skin. In contrast, dermatofibrosarcoma protuberans presents with a multinodular appearance with overlying epidermal atrophy imparting a taught, glossy appearance to the skin. All of these tumors are quite firm to palpation in contrast to the soft rubbery or gelatinous feel of a neurofibroma.