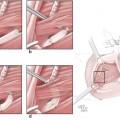
Fig. 17.1
Design of preoperative elbow lesion and incision

Fig. 17.2
Design of the parumbilical skin flap pedicled with inferior epigastric artery and vein

Fig. 17.3
The status after the completion of the surgery
2 The Osteosarcoma of Upper Humeral Shaft
2.1 Overview
Osteosarcoma is the most common type of primary malignant tumor. According to the literature, osteosarcomas account for 22% of malignant tumors and have a relatively high degree of malignancy; the prognosis is very poor, and the pulmonary metastasis occurs a few months later; the survival rate at 3–5 years after amputation is only 5–20%.
Osteosarcoma is the most common primary malignant bone tumor in childhood and adolescence. The osteosarcoma tends to occur in the long bone metaphysis, and now the osteosarcoma with lesions located in the diaphysis is called the diaphysial osteosarcoma; its incidence rate is low, accounting for only 0.52–9.50% of all osteosarcomas. The diaphysial osteosarcoma tends to occur in the long bones of limbs; most of them are found in the femur, followed by the humerus, fibula, and tibia. The osteosarcoma tends to occur in 15–20-year-old adolescents, while the age of onset of the diaphysial osteosarcoma is higher than that of other osteosarcoma, and the age of onset mostly exceeds 20 years.
2.2 Pathological Manifestation
In the 2002 WHO bone tumor classification, according to the pathological classification and pathogenic site, the osteosarcomas are divided into the general central type (including chondroblastic type, fibroblastic type, osteoblastic type, and eight subtypes derived from these three types), telangiectasia type, small-cell type, low-grade central type, cortical type, secondary type, juxtacortical type, periosteal type, and highly malignant superficial type; the pathological types of diaphysial osteosarcomas are also classified into the abovementioned respective subtypes. The osteosarcoma classification is more complex; the basic elements of the pathological diagnosis are the malignant sarcoma tumor cells and the neoplastic osteoid and bone formed directly by sarcoma cells, and the various subtypes have their characteristic pathological manifestation. The osteosarcomas in the humeral shaft can be divided into osteolytic type, osteoblastic type, and mixed type according to the manifestations of the bone damage on X-ray and MRI, and the osteoblastic type is commonly seen [5].
2.3 Clinical Characteristics
The osteosarcoma in the upper limb shaft has a lower clinical incidence rate, and the humerus is one of its most common locations of disease onset. The symptoms of osteosarcoma include progressive local pain, swelling and dysfunction, body weight loss, and anemia; the physical signs include tenderness, hard and tough masses, dark skin and varicose veins, and affected limb dysfunction. The laboratory tests show elevated alkaline phosphatase (1.5–4 Brinell units or 5–12 Guinness units in normal persons), and the higher value indicates more severe symptoms. The main clinical manifestations include pain and limb dysfunction. The main manifestations of X-ray and MRI include extensive bone damage, periosteal reaction, and easily observed soft tissue mass; the tumor bone and tumorlike calcification are still the main basis for imaging diagnosis. Comprehensive analysis of clinical X-ray, MRI, and pathological manifestations can accurately determine the diagnosis.
2.4 Diagnosis and Differential Diagnosis
Various subtypes of diaphysial osteosarcomas have their own characteristic pathological manifestations, but there are still similarities among them. The bone damages of the diaphysial osteosarcomas are more extensive, generally greater than 10 cm. The diaphysis has rich red bone marrow and more abundant blood supply. The tumor is more likely to spread within the medullary cavity of the diaphysis; therefore, the scope of tumor invasion is more extensive even the entire length of the diaphysis is involved. The diaphysial osteosarcomas are prone to periosteal reaction, and the tumor bone has many forms of manifestation, including spotlike, flocculent, needlelike, or ivory manifestation. Just like the metaphyseal osteosarcoma, the tumor bone and tumorlike calcification are still the main basis for the diagnosis of the diaphysial osteosarcoma with X-ray plain film. Andresen et al. divided the X-ray manifestations of the low-grade central osteosarcomas into four types: (1) osteolytic bone damage containing thicker bone crests; (2) osteolytic bone damage containing less incomplete slender bone crests; (3) simple osteosclerotic lesion; and (4) simultaneously combined with osteolytic bone damage and osteosclerosis. The low-grade central osteosarcoma is rare, accounting for only 1.96% of osteosarcomas, and is rarely located in the diaphysis; it is more difficult to diagnose relying solely on clinical and imaging manifestations, and it is required to integrate the histological manifestations of the characteristics of the benign lesion (spindle cells arranged in sarciniform and plexiform, rare mitotic figures, unobvious cell atypia) to make the diagnosis.
Most small-cell osteosarcomas show mixed bone damage, accompanied with periosteal reaction and soft tissue mass; the intramedullary and soft tissue ossifications are slighter and are easily misdiagnosed as Ewing’s sarcoma; the main identification points are that there exists characteristic regional bone-like tissue in pathologically damaged bone of the small-cell osteosarcoma. X-ray and MRI of the small-cell osteosarcoma show the osteolytic bone damage in the middle segment of the femur, thickened endosteum, layered periosteal reaction, needlelike tumor bone, and soft tissue mass. Because the needlelike tumor bone, periosteal reaction, and soft tissue mass are not the characteristic manifestations of the osteosarcoma, Ewing’s sarcoma may also have needlelike new bones with relatively consistent thickness and length; therefore, this type needs to be distinguished from Ewing’s sarcoma in onset age, location, imaging, and pathology. The onset age of low-grade central osteosarcomas is later than that of the general central osteosarcoma, and it is between 30 and 40 years old. The medical history is longer, and it can sustain for months to years.
Differential diagnosis of the diaphysial osteosarcoma: (1) Ewing’s sarcoma: It mostly occurs before the age of 30 years. Ewing’s sarcomas with small onset age mostly locate in tubular bones in the four limbs, and the femur is also the most common location of disease onset. The main imaging signs include intramedullary bone damage, periosteal reaction, and soft tissue mass; when the reactive bone sclerosis or residual bone fragments and needlelike new bone occur within the bone, it is difficult to distinguish it from the diaphysial osteosarcoma, especially the small-cell osteosarcoma; the identification between both depends on pathological examination. (2) Atypical osteomyelitis: It occurs mostly in children and young people; with the lack of obvious infection history, the medical history is usually longer. It mostly occurs in long bone diaphysis in the lower limbs, and is expanded and extended to the diaphysis, but it does not have dead bones, or the manifestation of dead bones is not obvious in most cases; the soft tissue swelling is also not obvious, and the surrounding bone and periosteal proliferation is slighter, or there is no periosteal proliferation. (3) Conventional intramedullary chondrosarcoma in long bones: The endosteum has scallop-shaped changes, and the arcuate or annular calcification and the surrounding partition-like enhancement pattern have certain characteristics. (4) Osteofibrous dysplasia: It is more difficult to distinguish it from the low-grade central osteosarcoma in the diaphysis in pathological and X-ray findings, but the osteofibrous dysplasia is less likely to break through the bone cortex and form a soft tissue mass; the invaded range in the bone marrow cavity is relatively limited, and the peritumoral soft tissue edema is relatively rare.
2.5 Treatment
2.5.1 Indications and Contraindications of Limb Salvage Surgery
- 1.
Main indications
- (1)
Enneking stage IA, IB, and IIA patients and some stage IIB chemotherapy-sensitive patients; the major blood vessels and nerves are not affected.
- (2)
If the local soft tissue conditions permit, the extensive resection can be achieved.
- (3)
There is no metastatic lesion or the metastatic lesion can be cured.
- (4)
The general condition is good, and the patient has a strong desire for limb salvage.
- (1)
- 2.
Contraindications: The recurrent tumors have huge tumor body, poor differentiation, and bad soft tissue condition, or when the major blood vessels and nerves surrounding the tumor are invaded by the tumor, it is advisable to perform amputation surgery.
2.5.2 Surgical Methods
The surgery may be carried out by means of extensive resection of proximal humerus alone, and when the lesion is close to the articular surface, a huge chunk of humerus together with scapula glenoid can be resected. The reconstruction methods vary with each individual. Young people need analgesia and stabilization, and thus the arthrodesis of shoulder may be considered, while the flail shoulder may be considered in elderly people.
The osteosarcoma patients undergoing surgery will be inevitably associated with the problem of tissue reconstruction. Currently the reconstruction techniques mainly include (1) bone tumor resection and arthrodesis, (2) bone transplantation, (3) tumor bone inactivation and reuse, (4) prosthesis replacement, and (5) composite limb salvage surgery. The selection of reconstruction materials is determined according to the experiences and habits of doctors, and the objective conditions, for example, the tumor bone shells in younger patients, are more complete and have a certain strength; the devitalized tumor bone shell and bone cement can be used for filling reinforcement, and the allogeneic bone stored in the bone bank at low temperature can also be selectively used for transplantation, but the patients should be informed that it’s prone to having an allograft reaction and leading to the limb salvage failure; the elderly people may select the artificial joint replacement. The soft tissue repair is most important; the wound infection and the necroses in the skin flap margin and skin flap should be reduced as far as possible; all these can lead to limb salvage failure. (6) When the osteosarcoma involves a large area of the skin, the pedicled or free skin flap can be used for repair, such as the latissimus dorsi myocutaneous flap and pectoralis major myocutaneous flap.
2.5.3 Postoperative Evaluation
The prognosis of traditional treatment methods (amputation and radiotherapy) is poor, and 5-year survival rate does not exceed 20%. The most important factor affecting the prognosis of osteosarcoma patients is the reaction degree of the tumor tissue to chemotherapy drugs, namely, the necrosis rate of tumor cells after chemotherapy, for patients with a necrosis rate of less than 90%; even if the chemotherapy regimen is changed, the prognosis is poor. Some scholars have reported that the patients with a tumor size of more than 150 mm3 have poor prognosis; the preoperative alkaline phosphatase and lactate dehydrogenase levels are also important for prognosis.
For the osteosarcoma patients without lung metastases, after preoperative and postoperative chemotherapy and appropriate surgical treatment, the cure rate is up to 60–80% at abroad; for the osteosarcoma patients treated in China, 5-year survival rate is 52%; 60% of patients have undergone limb salvage surgery, and the recurrence rate after limb salvage surgery is 12.5%.
2.6 Evaluation Method of Treatment and Its Standard
Surgery is the primary means for treatment of osteosarcoma. The purpose of surgical treatment is to safely resect the tumor and preserve the function as far as possible. For osteosarcoma patients, the local recurrence must increase the risk of metastasis, and therefore the selection of treatment scheme must consider the risk of local recurrence at first. To achieve the safety of the operation range, the surgical boundary should reach the extensive resection defined by the Enneking, including total resection of tumor tissue (should include biopsy channel) as well as the surrounding normal tissues within appropriate range which are not invaded, and the inadequate resection boundary will lead to increased local recurrence rate.
3 The Chondrosarcoma of the Upper Limb
3.1 Overview
The chondrosarcoma occurs in the soft tissue and originates from the chondrocyte or the malignant bone tumor of mesenchymal tissue differentiating into the cartilage, and its incidence rate accounts for about 20% of malignant bone tumors. Stout reported seven cases of chondrosarcoma and listed it as a separate disease entity at first in 1953. Istituto Ortopedico Rizzoli, Bone Tumor Center, summarized the data of 513 cases of chondrosarcoma encountered within 80 years; among them, there were only nine cases of chondrosarcoma within the ectosteal soft tissues, accounting for 1.7%, and the domestic literatures are mostly case reports.
This tumor tends to occur in middle-aged men, mostly in the lower limbs, especially in the thighs. Other frequent-onset locations include the calf, knee, hip, shoulder, ankle, hand, foot, groin, forearm, upper arm, and elbow.
3.2 Pathological Manifestation
The chondrosarcoma is the malignant bone tumor of mesenchymal tissue originating from the chondrocyte or differentiating into the cartilage, and it is often accompanied by matrix and myxoid degeneration, calcification, or ossification. It is mostly primary in origin, and it is secondary to enchondroma, osteochondroma, osteofibrous dysplasia, and Paget’s disease only in a few cases. It is divided into central (intramedullary) type and peripheral type according to pathogenic site, and the former is more common. It is divided into five types such as ordinary type, mesenchymal type, dedifferentiated type, myxoid type, and hyaline chondrocyte according to histology. It is divided into grade I–III according to the degree of differentiation: grade I is low-grade malignant, grade II is medial-grade malignant, and grade III is high-grade malignant. Grade I commonly shows cartilage calcification or ossification; relatively grade II shows less cartilage calcification or ossification; and grade III basically shows no cartilage calcification or ossification.
The pseudocapsule of mesenchymal chondrosarcoma is incomplete, the surface is lobulated or nonlobulated, the section surface is substantial, and it is dispersedly distributed with translucent cartilage lesions. It is mainly composed of undifferentiated mesenchymal cells and more maturely differentiated cartilage islands under microscopy; there is a clear boundary between the two, but the transient phenomenon of cell components is observed in some regions; that is, from undifferentiated mesenchymal cells to small spindle cells, the cartilage island is gradually formed. Under the electron microscope, the mesenchymal chondrosarcoma originates from undifferentiated mesenchymal cells, some are maintained in an undifferentiated stage, and some are differentiating toward the cartilage. Casadei considered that the myxoid chondrosarcoma has a complete pseudocapsule, and the section surface is gray-brown and transparent jellylike and may have bleeding and necrosis lesions; small, round, or long elliptic cells are observed under microscope, the nuclear chromatin is deeply stained, and the mitotic figure is rarely seen. The cells are separated by varying amounts of myxoid matrix. Under the microscope, it is observed that the dedifferentiated chondrosarcoma has a poorly differentiated sarcoma area on the basis of well-differentiated hyaline chondrosarcoma; there are a variety of histopathological types, such as fibrosarcoma, osteosarcoma, or malignant fibrous histiocytoma, and this type is rarer. The immunohistochemistry shows that S-100 protein and vimentin are positive, and the cytokeratin is negative.
3.3 Clinical Characteristics
The chondrosarcoma of the upper limb is usually demonstrated as a slowly growing painless mass at first; usually the patient only visits the hospital after the mass is significantly increased, and the patient feels pain a few weeks or a few years later.
Clinically, the onset age of chondrosarcoma is 11–60 years, the onset peak is 30–60 years, and the male to female ratio is 1.8:1. The onset age of dedifferentiated type is older, which tends to occur between 45 and 59 years in middle-aged and elderly people; the onset age of mesenchymal type age is smaller, which tends to occur between 10 and 29 years, with a median age of 26 years; the onset age of ordinary type tends to occur between 30 and 59 years; the patients less than 20 years are rarely seen; and the mucoid type occurs mainly in middle-aged men.
The clinical symptoms are mainly caused by local compression or invasion, including compressive and obstructive symptoms in the cavity-containing organs, an uncomfortable mass with no pain or dull pain in superficial parts, and no skin redness and swelling. The secondary lesion is that the painless mass is increased in short term and the pain occurs.
3.4 Diagnosis and Differential Diagnosis
3.4.1 Diagnosis
X-ray film shows soft tissue mass, and the calcification rate is 30%. The most common X-ray and CT signs of the mesenchymal type are the oval soft tissue masses with a clear boundary which contains a large number of irregular calcification, and the calcification is demonstrated as dotted and flocculent shapes, which is different from the granular or nodular calcification occurring in bone chondrosarcoma. The mucoid type has no calcification, with a lack of typical X-ray manifestations, and it is hard to be differentiated from other soft tissue masses in the plain film; due to rich mucus, CT shows a low density homogeneous mass. In some cases, CT can not only find the soft tissue mass and determine the invasion range but also find calcification-ossification shadows which cannot be shown on X-ray film, which are mostly point-like, circular, or semicircular; CT is now considered as the most effective means of imaging in early diagnosis of this disease. In recent years, MRI is also widely used to diagnose bone tumors and shows the muscle signal on T1-weighted image and high signal on T2-weighted image, of which both the calcification and ossification are low signals. When the angiography is carried out, the outline of the mucoid chondrosarcoma and the relationship of the reactive vascular proliferation in the adjacent soft tissue with the blood vessels and nerves can be clearly shown, and the tumor itself is not obviously developed, while the mesenchymal chondrosarcoma shows excessive proliferation of tumor blood vessels. Some patients may have signs of erosion of adjacent bone [6].
3.4.2 Differential Diagnosis
The chondrosarcoma should be differentiated from the following diseases:
- 1.
Enchondroma. The ordinary chondrosarcoma in tubular bones should be differentiated from the enchondroma. The enchondromas tend to occur in the short tube bones and are often multiple, the bone cortex is expanded and thinned, the typical case has candied fruit-like changes, and the enchondroma occurring in the long bone is mostly demonstrated as the limited calcification without corrosive destruction of the bone cortex. No soft tissue mass is formed around the enchondroma, and there is often no pain symptoms.
- 2.
Osteoclastoma and chondroblastoma. The clear-cell chondrosarcoma should be differentiated from the osteoclastoma and chondroblastoma. The osteoclastoma mostly has bubble-like bone destruction and has no hyperostosis, osteosclerosis, and calcification; the fluid-fluid levels may occur on MRI; the onset age of chondroblastoma is younger; the chondroblastoma mostly occurs in the vicinity of the epiphyseal plate; and the size is generally less than 5 cm.
- 3.
Chordoma and meningioma. The chondrosarcoma occurring in the skull, especially the myxoid chondrosarcoma, should be differentiated from the chordoma and meningioma. The chordoma tends to occur in the slope and is located in the middle area and mostly shows osteolytic and expansive bone damage, in which the residual bone instead of bone calcification is observed; and the chondrosarcoma mostly biases toward one side and occurs in the binding region of the skull, and there may be typical calcification; the small interatrial septum-like enhancement is observed within the tumor after enhanced scan.
- 4.
Osteosarcoma and neurogenic tumors. The chondrosarcoma occurring in the parosteal area and soft tissue should be differentiated from the osteosarcoma and neurogenic tumors. The onset age of the osteosarcoma is mostly younger, and the periosteal reaction is heavier, the Codman triangle and the tumor bone often appear, the soft tissue masses mostly have equal density, and the clinical symptoms are more obvious. The chondrosarcoma is mostly the low-density mass, the characteristic calcification is commonly seen, the periosteal reaction is lighter, and some neurogenic tumors may have calcifications, but that are mostly flocculent and patchy calcifications, which is different from the calcification characteristics of the cartilaginous tumors.
- 5.
Others. The extraskeletal chondrosarcoma should be differentiated from the soft tissue chondroma, chondromyxoid fibroma, chondromyxoid fibroma, chordoma, myxoid lipoma, malignant hemangiopericytoma, and myositis ossificans. Because the incidence rate of this tumor is low, there is a certain degree of difficulty in diagnosis.
3.5 Treatment
3.5.1 Indications and Contraindications of Limb Salvage Surgery
- 1.
Main indications
- (1)
Enneking stage IA, IB, and IIA patients; some stage IIB chemotherapy-sensitive patients, and the major blood vessels and nerves are not affected.
- (2)
If the local soft tissue conditions permit, the extensive resection can be achieved.
- (3)
There is no metastatic lesion or the metastatic lesion can be cured.
- (4)
The general condition is good, and the patient has a strong desire for limb salvage.
- (1)
- 2.
Contraindications. The recurrent tumors have huge tumor body, poor differentiation, and bad soft tissue condition, or when the major blood vessels and nerves surrounding the tumor are invaded by the tumor, it is advisable to perform amputation surgery.
3.5.2 Surgical Methods
Although the non-characteristic clinical and X-ray manifestation can delay the diagnosis and treatment, the treatment method is also an important prognostic factor. The tumor is mainly treated by surgical resection, the recurrence rate after intracystic or marginal resection is very high (30–100%), and the rate of postoperative recurrence and metastasis is 20–60%.
The important measure of the surgical resection is that the tumor is resected en bloc at the best surgical boundary outside the tumor. The selection of resection plane during surgery must be determined according to preoperative Enneking staging. After chemoradiotherapy, the tumor is shrunk, and the boundaries are clear, which helps achieve the goal of radical resection of tumor. The range of extensive resection should include the tumor body, envelope, reaction zone, and the surrounding adjacent 10-cm-thick normal tissue, and the resection should be performed in this normal tissue structure as far as possible. For the tumors with highly aggressive biological behavior, which don’t receive chemotherapy or are insensitive to chemotherapy, the cuneiform plane should be at 6 cm outside the lower boundary of the tumor (determined according to preoperative MRI), and the resection range of the soft tissue should be 2–3 cm outside the reaction zone. The tumor patients who are sensitive to chemotherapy can be treated with resection with smaller surgical boundary; the femoral resection should be carried out at 3 cm under the lower boundary of the tumor, and the soft tissue resection is performed at 1 cm outside the tumor. Generally, it is believed that the myxoid chondrosarcoma is a low-grade malignant tumor; it grows slowly and has a good prognosis. The metastasis rate is low, even if lung metastasis occurs; the metastasis focus can be resected, and the extensive resection can be performed; while the malignancy degree of the mesenchymal chondrosarcoma is high, it can be easily metastasized to the lungs through blood channels; in a few cases, it is metastasized to the regional lymph nodes, the prognosis is poor, and the radical resection should be carried out. Because the tumor site is mostly located outside the compartment, therefore it is often difficult to carry out limb salvage surgery in the patients with mesenchymal chondrosarcoma. When the tumor involves the skin, the pedicled or free skin flap can be used for repair.
3.5.3 Postoperative Evaluation
The statistics by Amir showed that the recurrence may take place at 2 months to 15 years after surgery (with an average of 2.6 years) and the metastasis may take place at 4 months to 17 years after surgery, namely, some patients may have recurrence and metastasis many years later; therefore, the tumor patients must be followed up for a long time. Although the chemotherapy and radiotherapy may be used as adjunctive therapy of this tumor, their exact effects are not yet clear.
3.6 Evaluation Method of Treatment and Its Standard
The chondrosarcoma is a malignant bone tumor with relatively slow clinical progression and low metastasis rate, and the purpose of clinical basic treatment is to remove the tumor as thoroughly as possible and prevent recurrence; the imageological examination, especially CT and MRI, provides a reliable basis for proper clinical diagnosis, guiding treatment, and postoperative reexamination.
4 The Clear-Cell Sarcoma of the Upper Limb
4.1 Overview
The clear-cell sarcoma (CCS) occurring in the limbs is a clinically extremely rare soft tissue malignant tumor and is also known as soft tissue melanoma. Enzinger firstly proposed the clear-cell sarcoma in 1965. In the new edition of WHO soft tissue tumor classification, the soft tissue clear-cell sarcoma is used and listed as the tumor with an uncertain classification.
The clear-cell sarcoma occurs mainly in the tendon and aponeurosis of the distal limb in young and middle-aged people. Related studies have found that the vast majority of clear-cell sarcomas contain melanin; Chung and Enzinger also called it as the soft tissue malignant melanoma in 1983. It is a malignant soft tissue sarcoma with a lower incidence rate, accounting for about 1% of soft tissue sarcomas, and the mortality rate is between 39% and 74%.
4.2 Pathological Manifestation
There are two kinds of views on the histological origin of clear-cell sarcoma: one view is that the tumor cells are similar to the synovial membrane; therefore, it is considered as a kind of synovial sarcoma, and another view is that the tumor cells contain melanin; thus, it is considered that the clear-cell sarcoma derives from the neural crest. Clinically, this tumor is more commonly seen in young and middle-aged people. The incidence rate of this kind of tumor in Asian populations is relatively lower, and therefore there are few domestic reports on clear-cell sarcoma in the four limbs, especially in the upper limbs.
4.3 Clinical Characteristics
The clear-cell sarcoma in the upper limbs occurs mainly in the distal limbs; it is rarely seen in the head, neck, and trunk, and it is mainly located in the deep tissues, involving the tendons and aponeurosis, generally not involving the skin, but the larger tumors can invade the skin. The onset of tumor is insidious; sometimes the tumor develops slowly and often has no accompanying symptoms. When the patient seeks treatment, frequently it has been a while since the onset of the tumor. Approximately 50% of patients have a history of trauma at the tumor site.
The main clinical manifestation is the local mass in the upper limbs, which may have pain and tenderness, with less redness and swelling. The tumor texture is harder, with clear boundary. This tumor is often solitary, and may also be multiple, often adheres to the tendon, and is prone to recurrence and metastasis; the regional lymph node metastasis is commonly seen, the lymph node metastasis in early stage is one of the characteristics that makes it different from other soft tissue sarcomas; as the sites of distant metastasis, the lung is most commonly seen, followed by the liver, bone, and brain.
The mode of the metastasis of clear-cell sarcoma is mainly the lymphatic metastasis; the patients who are found with regional lymph node invasion before surgery should also undergo regional lymph node dissection. The patients after tumor resection are prone to recurrence, and the local recurrence rate is 50–84%. The emergence of regional lymph node metastasis is more common than other soft tissue sarcomas, and the regional lymph node metastasis rate in ordinary soft tissue sarcomas is about 8%, while the regional lymph node metastasis rate in clear-cell sarcomas is 33–53%. The most common site of distant metastasis is the lung, and the occurrence rate is 44–53%. The sentinel lymph node biopsy is definitely helpful in early detection of tumor metastasis.
4.4 Diagnosis and Differential Diagnosis
At present, the diagnosis of clear-cell sarcoma mainly depends on the pathological examination, which is characterized as follows: it is observed by the naked eye that the texture is generally harder, nodular, or lobulated; in most cases, it closely adheres to the tendons and aponeurosis, and it is commonly seen that the surrounding muscle or subcutaneous adipose tissue is invaded, but the local skin is generally more complete. The section surface of the tumor is gray-white, and sometimes the spots or glue-like mucus degeneration is visible. The epithelioid and spindle cells can coexist in the same tumor, and the transition is observed. Microscopically, most tumor cells are irregularly polygonal or spindle-shaped and are arranged densely in pieces or nests and are separated by fibrous tissue. The cells are round or spindle-shaped, with clear nuclear membrane and large and obvious nucleoli, and the cells are basophilic; in the cytoplasm, there is an aggregation of a lot of glycogen, swelled mitochondria, and vesicles with interface membrane, and a large number of ribosomes, polysomes and rough endoplasmic reticulum, and the melanosomes in different periods are observed. Some tumors contain polynuclear giant cells, which are focally distributed, with a rosette-like arrangement. Under the electron microscope, some tumor cells contain melanin granules. The most applied immunohistochemical indicators are S-100 and HMB-45 staining, the positive rate of S-100 expression is higher, and the specificity of HMB-45 staining is higher.
Related posts:
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
 Neuroma Model
Neuroma Model
 Defect Repairs After Resections of Laryngeal Cancer, Hypopharyngeal Cancer, and Cervical Esophageal Cancer
Defect Repairs After Resections of Laryngeal Cancer, Hypopharyngeal Cancer, and Cervical Esophageal Cancer
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


