Fig. 4.1
Direct suture. (a) Defect after tumor surgery. (b) Location. (c) Sew up the palpebral margin. (d) Completion
1.2 The Method for Vicarious Suture of Anterior and Posterior Layers of the Eyelid
This method is also applicable to the full-thickness defects. The surgical procedure is as follows:
- 1.
Trim the wound margin to make it triangle shaped, and incise open along the dotted line to form two lobes such as the anterior lobe and the posterior lobe (Fig. 4.2a).
- 2.
On one side of the wound, remove downward from the eyelid margin a strip of tissue of eyelid anterior layer with a width of 2–3 mm, and then remove the corresponding tissue of eyelid posterior layer in the opposite wound margin (Fig. 4.2b).
- 3.
Perform a mattress suture; insert the needle, respectively, at the conjunctival surface at one side of the tissue of eyelid posterior layer with both ends of the suture line tissue; pass through the tarsus, penetrate out of the skin surface on the other side of the anterior layer, and pass through a sheet rubber; and then incise open the lateral canthus by two times the length of the defect according to the size of the defect area (Fig. 4.2c).
- 4.
Ligate the mattress suture line on a small piece of sheet rubber. The suture line penetrates through the deep tissue in the outer canthus, and the interrupted suture is performed (Fig. 4.2d).
- 5.
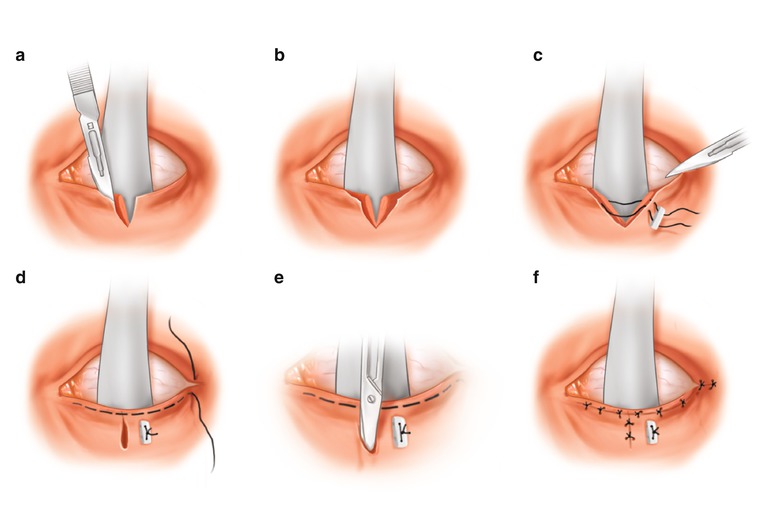
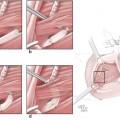
Fig. 4.2
The method for vicarious suture of anterior and posterior layers of the eyelid. (a) Incise open the lower eyelid along the dotted line. (b) Excise anterior skin layer of eyelid on one side, excise posterior tarsal plate layer of the eyelid on the other side. (c) Sew up posterior tarsal plate layer. (d) Horizontally sew up the anterior lobe and the posterior lobe. (e) Vicarious suture the vertical skin incision. (f) Completion
2 Repair of Medium or Large Upper Eyelid Defect
2.1 Cutler-Beard Method
This method is suitable for long and thin upper eyelid defect, and the surgical procedure is as follows:
- 1.
Cut through the eyelid paralleling to the eyelid margin at the site with a distance 3–4 mm from the lower eyelid margin, and the length is equal to that of the upper eyelid defect. Along both ends of the transverse incision, incise downward the full thickness of the eyelid vertically to the eyelid margin; cut straightly toward the bottom of the lower eyelid dome, and the length is about 15 mm. Finally, the lower eyelid flap is formed (Fig. 4.3a).
- 2.
Separate the skin and subcutaneous tissues from the muscle in the lower eyelid flap, and separate the conjunctiva from the muscle, which leads to complete looseness between the conjunctiva and skin in order to successfully pull it up to the upper eyelid defect. The lower eyelid margin becomes a “bridge” with both ends connected to the canthus.
- 3.
Pull upward the lower eyelid flap from the area under the “bridge”-shaped eyelid margin, and transplant it in the upper eyelid defect (Fig. 4.3b). The conjunctiva is sutured with the muscle and the remaining posterior lobe of upper eyelid, and the skin and muscle are sutured interruptedly. The approximating suture of skin and conjunctiva in the lower eyelid margin wound is performed.
- 4.
The compression bandaging is performed for 2–3 days, and the stitches are taken out 7 days later. After 2 months, at the same height of the healthy eye, the tarsus flaps which are cut off and implanted at the inner and outer canthus are connected, and the wound in the eyelid margin is sutured; the broken end of transplant flap under the “bridge” is restored to its previous position (Fig. 4.3c). The lower eyelid margin incision is separated again, and an apposition suture is performed.
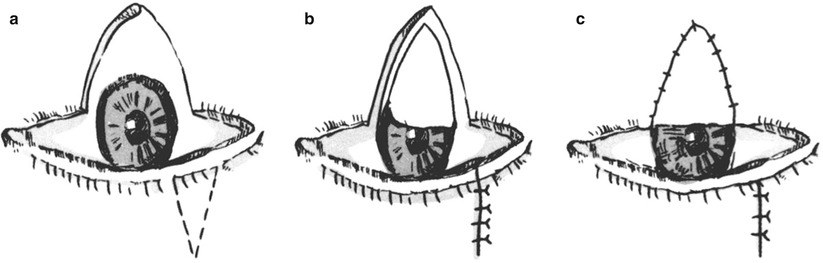
Fig. 4.3
Cutler-Beard method. (a) The lower eyelid is cut through transversely at the site with a distance 3–4 mm from the lower eyelid margin, and the lower eyelid flap is formed. (b) The lower eyelid flap is passed through the “bridge”-shaped eyelid margin and is transplanted onto the upper eyelid defect. (c) The transplant flap is cut off at 2 months after surgery, then the palpebral fissure is made, and the transplant flap under the “bridge” is restored to its previous position
2.2 Composite Transplantation Method
This method is suitable for patients with upper eyelid full-thickness defects, and the surgical procedure is as follows:
- 1.
Take out a full-thickness tissue block in the lower eyelid, whose width doesn’t exceed 1 cm, and it shows a triangular shape (Fig. 4.4a).
- 2.
Fig. 4.4
Composite transplantation. (a) A full-thickness tissue block in the lower eyelid is taken out according to the dotted line. (b) The wound in donor site is closed and sutured directly, and the margin of the upper eyelid defect is trimmed. (c) After the transplant block is placed in the upper eyelid, the vicarious suture of anterior and posterior layers is performed
2.3 Repair Method with the Ortho-position Skin Flap
Case I
This is a patient with simple eyelid skin defect, and the defect can be repaired with the ortho-position skin flap (Fig. 4.5).
Fig. 4.5
Case I. (a) The right upper eyelid basal cell carcinoma. (b) The tumor resection range and skin flap design. (c) Upper eyelid defect after tumor resection. (d) The eyelid shape is good at 10 days after surgery
2.4 Forehead Flap
This method is suitable for the repair of the upper or lower eyelid skin defect due to tumor resection.
The blood supply of the forehead flap includes two systems such as the frontal branch of the superficial temporal artery as well as the supraorbital artery and supratrochlear artery, and there is a netlike distribution of rich anastomosis branches between two systems of blood vessels. In general, there are concomitant venous veins of the same name for venous return. Any system of blood vessels can be taken as the supplying vessels, and both can feed and ensure the survival of the skin flap.
The forehead flap can be used for repair of upper and lower eyelid defects, which is appropriate to take the superficial temporal artery as the pedicle for the lower eyelid; the superficial temporal artery or the supratrochlear artery can be taken as the pedicle for the upper eyelid according to the defect site.
Case II
This is a patient with upper eyelid defect, and the forehead flap is used for repair (Fig. 4.6).
Fig. 4.6
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
 Neuroma Model
Neuroma Model
 Tissue Engineering and Oncological Surgery
Tissue Engineering and Oncological Surgery




Case II. (a) The upper eyelid mass and skin flap design. (b) The defect after mass resection. (c) The forehead flap is passed through the subcutaneous tunnel to repair the eyelid defect
Related posts:
Microcirculation Model for Invasive Animal Monitoring
Composite Osseomusculocutaneous Thymus Allotransplantation Model
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Neuroma Model
Tissue Engineering and Oncological Surgery
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
