The purpose of this article is to provide the plastic, dermatologic, oculoplastic, and facial plastic surgery communities with anatomic and embryologic evidence to support the use of the deep-plane technique for optimal treatment of midfacial aging. A detailed description of the procedure is provided with insights into anatomic landmarks, technical nuances, and alternative approaches to facial variations to allow safe and consistent performance of this technique.
Key points
- •
The platysma muscle/superficial musculoaponeurotic system/galea is the continuous superficial cervical fascia encompassing most of the facial fat, and this superficial soft tissue envelope is poorly anchored to the face.
- •
The deep-cervical fascia binds the structural aspects of the face and covers the facial nerve and buccal fat pad.
- •
Facial aging is mainly due to gravity’s long-term effects on the superficial soft tissue envelope, with more subtle effects on the deeper structural compartments.
- •
The deep-plane is the embryologic cleavage plane between these fascial layers and is the logical place for midfacial dissection.
- •
The deep-plane allows access to the buccal fat pad for treatment of jowling.
- •
Soft tissue mobilization is maximized in deep-plane dissections and requires careful hairline planning.
- •
Flap advancement creates tension only at the fascia level allowing natural, tension-free skin closure, and long-lasting outcomes.
- •
The deep-plane advancement flap is well vascularized and resistant to complications.
Introduction
Methods used to rejuvenate the midface are varied and often depend on the perspective created by the surgeon’s specialty training. Theories and beliefs about the cause of facial aging will also influence a surgeon’s particular preference or prejudice. The literature is filled with controversy surrounding the cause of midfacial aging. Recent literature focuses on fat/volume loss as the principle contributor to midface aging, theoretically validating the use of facial volume enhancement as the main treatment modality.
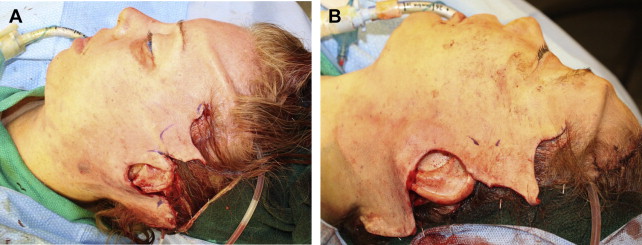
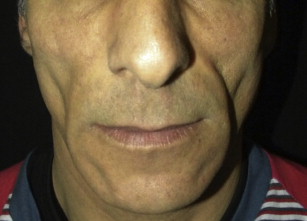
But facial palpation and intraoperative views of the facial soft tissues after sub–superficial musculoaponeurotic system (SMAS) dissection and mobilization, used as the facial rejuvenation technique, reveal excessive soft tissue redundancy ( Fig. 1 ). Such photos, combined with operative experience, prove the long-term effects of gravity’s downward pull on the poorly anchored superficial soft tissue envelope as the central factor in facial aging. True fat/volume loss is evident in patients suffering from HIV wasting syndrome ( Fig. 2 ) but a sunken appearance is observed and facial palpation does not reveal excessive soft tissue redundancy, further debunking the volume theory of facial aging.
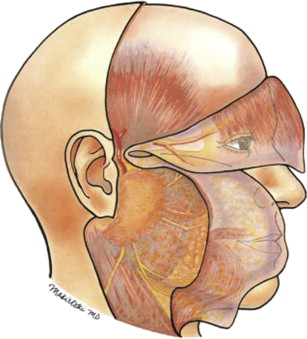
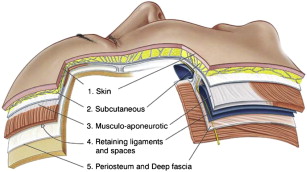
Techniques aimed at reversing gravity’s effects have evolved as the authors’ understanding of facial anatomy has progressed. Mitz and Peyronie defined the superficial cervical facial fascia in 1976, demonstrating the SMAS to be a fibromuscular extension of the platysma muscle. Skoog advanced facelift techniques by defining the significance of the sub-SMAS dissection. Further improvement was made by Hamra in 1990 with his description of the deep-plane rhytidectomy. The deep plane of the face is defined as the embryologic cleavage plane separating the superficial soft tissue envelope from the deeper structural aspects of the face bounded by the deep cervical fascia ( Figs. 3 and 4 ). Dissection of the midface in the sub-SMAS/deep plane creates advantages that allow for significantly improved outcomes in face lifting. This approach enables direct lysis of the zygomatic cutaneous ligament, which is the major facial retaining ligament; direct assessment and treatment of issues such as pseudoherniation of buccal fat and its influence on jowling; and mobilization of most of the facial fat. Additionally, the deep-plane dissection confines tension to the platysma/SMAS fascia, allowing for a tension-free skin closure, minimizes complications, and results in a natural rejuvenation.
Anatomy
By understanding the relevant midface anatomy and embryology, the authors’ preference for the deep-plane rhytidectomy technique and its safe performance becomes evident. Initially viewing the layers of the face (see Fig. 4 ), we see the SMAS is the deep layer of the superficial soft tissue, with most of the facial fat distributed homogeneously superficial to this layer. This embryologic boundary is contiguous from the platysma in the neck to the galea in the forehead (see Fig. 3 ). Below this layer is the superficial layer of the deep cervical fascia, covering all the deeper embryologic structures ( Fig. 5 ) such as the masseter muscle, facial nerve, and buccal fat pad. The potential space located between these layers represents the embryologic cleavage plane of the midface and defines the deep plane. Dissection in this potential space is relatively avascular, and the facial nerve is securely protected by the deep cervical fascia. Additionally, the SMAS fascia fuses with the superficial layer of the deep cervical fascia at the parotid gland and is poorly defined superiorly over the facial mimetic muscles such as the zygomatic and orbicularis muscles. Thus, most of the malar fat pad sits on this superior group of facial mimetic muscles. Crossing through these planes are the 2 facial ligaments, at the body of the zygoma are the zygomatic cutaneous ligaments (McGregor’s patch), and inferiorly on the medial aspect of the mandible are the mandibular ligaments, which are the sole anchors of the facial soft tissue envelope ( Fig. 6 ). The deep plane is very well defined inferiorly along the masseter muscle because of the presence of platysma muscle in the SMAS fascia. Superiorly, the deep plane is more poorly defined, because the fascia thins out at the level of the facial mimetic muscles.
Patient evaluation
Evaluation of a surgical candidate should include the standard medical clearance for a patient undergoing general anesthesia; the authors prefer that the patient be intubated under a propofol-based anesthetic. Often midface procedures are combined with brow lift, eyelid, and neck procedures.
Physical evaluation should be based on the specific combination of procedures to be performed. The presence and degree of the nasolabial folds, jowling, festoons, and facial dimples should be defined for the deep-plane midface lift.
From the perspective of the facial plastic surgeon, the importance of defining face type by palpation of the facial soft tissue cannot be overemphasized. Compliant faces will often manifest the effects of gravity at an earlier stage and create more soft tissue mobilization, thus requiring careful hairline planning. Stiff, noncompliant faces can be more difficult to dissect, but these typically will maintain their outcomes for a longer period of time. Thicker soft tissue will require more lateral soft tissue contouring when the flap is mobilized. The deep plane will be more proximal to the subcutaneous plane in thin faces.
Complete neurologic examination should document both trigeminal nerve status and facial nerve function. Photographs should document both static and dynamic images in frontal, three-quarter, and lateral views. Ear position and shape, facial asymmetries, and hairlines should be documented. Dynamic images should document patterns of muscle action ( Fig. 7 ).
Patient perspective
Patients desire the best outcome with the least process. Most patients must be able to be cosmetically presentable in public within 2 weeks. An individual’s aesthetic goals should be balanced with their stage of aging so the best treatment plan can be defined over time. Risks and benefits should be discussed before any contemplated procedure. Minimally invasive procedures and their limitations should be presented as alternatives. Before and after photographs of the contemplated procedure are helpful to establish realistic expectations of outcomes.
Surgical procedure
The importance of detailed surgical planning is crucial in aesthetic surgery. Intraoperative access to preoperative photographs is also essential. Although most of the deep-plane midface lifts are combined with other procedures, the authors describe only the midface lift portion of the procedure in the later discussion.
Anesthesia
The authors prefer to do the procedures under a propofol-based general anesthetic. Bleeding is also controlled throughout the procedure by a surgical field injection of a 1:1 mix of 1% lidocaine with 1:100,000 epinephrine, with 0.5% bupivacaine with 1:200,000 epinephrine, combined with hypotensive anesthetic techniques when appropriate. Perioperative antibiotics covering skin flora and one dose of intravenous steroids are given before incision. Muscle relaxants are not used except for a short-acting agent for induction into anesthesia.
Incision
Once the patient has been anesthetized, the authors proceed to cut the hair and mark accordingly ( Fig. 8 ). A retrotragal incision is typically used in women because the deep-plane procedure avoids tension on the incision lines, maintaining normal ear and tragal architecture. In men, pretragal incisions are necessary to avoid moving hair-bearing skin on to the tragus. Because there is such a great degree of soft tissue mobilization using the deep-plane technique, even in younger patients, the authors prefer to use temporal hairline incisions to avoid superior and posterior movement of the temporal hair tuft (see Fig. 1 ). The necessity of postauricular incisions will be defined by whether any neck improvement is being sought and by the anticipated degree of soft tissue movement. In general, the authors, based on their prediction of soft tissue mobilization, design the postauricular limb more superior, with a more acute angle (compared with the antihelix), for patients with relatively compliant soft tissue. The postauricular limb is more inferior, with a more obtuse angle, for patients who have less compliant soft tissue or with revision cases. The greater the degree of soft tissue mobilization in the midface, the greater is the need for extending incisions to accommodate the excision of redundant soft tissue.
Related posts:
 An Algorithmic Approach to Multimodality Midfacial Rejuvenation Using a New Classification System for Midfacial Aging
An Algorithmic Approach to Multimodality Midfacial Rejuvenation Using a New Classification System for Midfacial Aging
 Dark Circles
Transconjunctival Lower Lid Blepharoplasty with and Without Fat Repositioning
The Management of Festoons
The Transeyelid Midface Lift
Dark Circles
Transconjunctival Lower Lid Blepharoplasty with and Without Fat Repositioning
The Management of Festoons
The Transeyelid Midface Lift
 Transtemporal Midface Lifting to Blend the Lower Eyelid-Cheek Junction
Transtemporal Midface Lifting to Blend the Lower Eyelid-Cheek Junction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


