Debridement of Infected Bone of the Foot and Ankle
Michael C. Holland
Scott L. Hansen
DEFINITION
Osteomyelitis of the foot and ankle is defined by bacterial or less commonly fungal infection of bones of the lower third of the leg and foot.
Spectrum of severity can range from chronic, indolent infections to acute, suppurative infections resulting in sepsis.
Often resulting from existing soft tissue wound extending deep to underlying bone; however, seeding (eg, from bacteremia), direct inoculation (eg, trauma, puncture wounds), or healing of prior soft tissue defects can result in isolated osteomyelitis in the absence of soft tissue signs or symptoms.
Frequently associated with hardware and prior fractures necessitating removal or replacement of hardware.
The management of acute osteomyelitis is primarily medical, whereas the management of chronic osteomyelitis is mainly surgical in combination with antibiotic therapy.1
ANATOMY
The ankle is formed by the distal aspect of the tibia (medial) and fibula (lateral) articulating with the talus of the foot.
The foot is composed of 26 bones functionally homologous to bones of the hand and wrist.
The hindfoot is composed of the talus, which is seated on the calcaneus.
The midfoot articulates with the bones of the hindfoot and is composed of the cuboid navicular and three cuneiform bones (medial, intermediate, and lateral).
The forefoot is composed of the 5 metatarsal bones and 14 phalanges.
Two sesamoid bones underlying the first toe metatarsal phalangeal joint also are present in adults, with infrequently found accessory sesamoid bones at other joints.2
PATHOGENESIS
Infection most often arises from soft tissue wounds, open fractures, complications from orthopedic reduction of closed fractures, hematogenous seeding from bacteremia or endocarditis, or inoculation from trauma
PATIENT HISTORY AND PHYSICAL FINDINGS
History of diabetes mellitus, vascular insufficiency, venous hypertension, peripheral neuropathy, immunodeficiency, prior fracture, presence of hardware, prior surgery, and prior podiatric procedures are important to identify preoperatively in order to determine whether or not adjuvant therapy may be beneficial to precede operative intervention.
Diminished sensation, paresthesias, and claudication are symptoms that may indicate the presence of these above comorbidities.
Presence of open wounds with or without visible bone, erythema, fluctuance, and bony tenderness can indicate active infection.
Decreased Semmes-Weinstein monofilament test, prior scars, palpable hardware, and venous ulceration are physical exam findings that may indicate higher-risk populations for developing osteomyelitis.
IMAGING
Three-view plain radiographs of the foot and ankle are the first test to order, and will help give clear definition of bony anatomy, presence of hardware or radiopaque foreign bodies, and can detect subtle changes of osteomyelitis as early as 10 to 14 days but typically requires 3 weeks of active infection before changes will be found.3
CT scan is useful for demonstrating extent of osteomyelitis and may detect radiologic changes earlier than plain radiographs; however, sensitivity is limited at around 67%5 and may have findings obscured by hardware artifact. Utility may be found in ability to evaluate extent of disease and to create three-dimensional reformats for reconstructive planning.
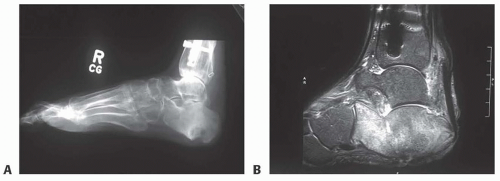
FIG 1 • A. Radiograph of the right foot demonstrating periosteal reaction of the calcaneus indicating osteomyelitis. B. Corresponding MRI of the right foot demonstrating the extent of calcaneus osteomyelitis.
MRI is the most sensitive and specific modality for diagnosis of osteomyelitis, as early as 3 to 5 days (FIG 1B).6,7Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree