BOTULINUM TOXIN
I. BACKGROUND
Botulinum toxin was first discovered and implicated over 100 years ago as a cause of muscle paralysis. It was not until 1946 however that Dr. Edward Schantz was able to isolate and purify the toxin for therapeutic use. The protein molecule, produced by the anaerobic bacterium Clostridium botulinum, is a neurotoxin. The molecule is composed of the neurotoxin itself along with large surrounding protective proteins.
Botulinum toxin blocks the release of acetylcholine at the neuromuscular junction which is critical for neuromuscular transmission. Specifically, botulinum toxin serotype A exerts its effect by cleaving SNAP-25 (synaptosomalassociated protein), a protein required for acetylcholine release. Because of this unique mechanism of action, botulinum toxin was originally used as a treatment for patients with muscular spasm, such as blepharospasm. In 1988, Drs. Jean and Alastair Carruthers made a key observation that periorbital rhytides improved in patients treated for blepharospasm. This observation led to the Carruthers’ seminal study in 1992 regarding the cosmetic application of botulinum toxin. Since then, the use of botulinum toxin in noninvasive facial rejuvenation has grown tremendously. Dermatologists now commonly use botulinum in the treatment of hyperhidrosis and dynamic rhytides of the forehead, periorbital area, midface, perioral area, and neck. In fact, botulinum toxin injection is the most common nonsurgical cosmetic procedure performed today. Botulinum toxin has consistently been shown to be a safe and effective treatment when injected by knowledgeable and experienced practitioners.
II. CLINICAL PRESENTATION
The typical patient presenting for botulinum toxin injection can range from the young to the elderly. Traditionally in cosmetic use, the patients were often characterized as middle-aged females, but with the significant increase in its popularity, botulinum toxin is now utilized over a much broader demographic. Botulinum toxin injections are used to treat dynamic rhytides or wrinkles formed by muscular contraction. Thus, at rest, wrinkles may not be apparent as it is the contraction of muscles which lead to these lines. The three most commonly treated areas are the glabella, crow’s feet, and forehead. There are many other injection points, including the lower face and neck, which can be treated as well.
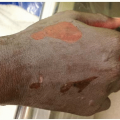
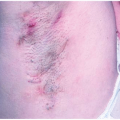
For patients with hyperhidrosis, obvious sweating may be appreciated at the time of presentation but oftentimes, the patient is only able to give a history of excessive sweating. One survey estimated that up to 2.8% of the US population may be affected. Primary hyperhidrosis is defined as excessive sweating lasting for 6 months or more without an apparent cause and has at least two of the following features: bilateral symmetric sweating, impairment of
daily activities, frequency of greater than one episode a week, positive family history, onset before age 25, and cessation of sweating while asleep.
III. WORKUP
Perhaps the most important part of the patient’s visit is the preprocedural assessment. It is crucial to assess the patient’s expectations and to clearly define the risks and benefits. While the risks of botulinum toxin in cosmetic use are exceedingly rare, when they do occur, the temporary effects can cause significant morbidity in some patients. It is recommended that preprocedural pictures be taken as they can be helpful to show a patient the change that has been made by the procedure.
The clinician should assess the severity of the dynamic rhytides. Some patients have naturally weaker muscles, so the dosing should be adjusted or treatment of that area may be skipped completely. The muscles of the face have a complex interplay with one another so weakening one muscle too much in relation to others can lead to poor cosmetic results if not done correctly. When significant rhytides are noted at rest, a combination treatment with botulinum toxin and soft-tissue augmentation injection or laser resurfacing should be considered. Botulinum toxin injection will help soften wrinkles and prevent the formation of deeper lines formed by dynamic motion, while fillers or lasers can correct static rhytides.
In general, botulinum toxin injection is contraindicated in those with a hypersensitivity to the product or who have an ongoing infection at the injection site. Botulinum toxin injections should also be avoided in women who are pregnant or lactating and those with preexisting neuromuscular conditions.
With hyperhidrosis, the diagnosis relies more commonly on a detailed patient history. To save time, patients can be given a questionnaire to quantify their symptoms on a Hyperhidrosis Disease Severity Scale or a Dermatology Life Quality Index. The minor starch iodine test and gravimetric analysis are more cumbersome tests to perform and used less commonly today. In some cases, insurance companies may subsidize all or part of the treatment if indicated by the hyperhidrosis disease severity scale.