CHAPTER 42 Correction of the deviated septum
Physical evaluation
• Thorough history: A detailed patient history including history of nasal trauma, previous nasal surgery, airway complaints, allergies, and age is obtained. A negative history of airway obstruction is not a reliable indication of a patent airway, since the patient has no basis for comparison.
• Facial analysis: The nose and face are evaluated in 3 dimensions and findings are confirmed with soft tissue cephalometric analysis of life-size photographs. This is performed in order to assess symmetry of the nose and its relationship to other facial structures. Asymmetry may be present in other facial features, thus affecting the global evaluation of the face. The AP view of the face is also used to evaluate the dorsal nasal aesthetic lines as well as the width of the nasal dorsum.
• Often, the nasal bones follow the direction of the deviated septum, however these structures may move independently. Deviation of the lower nose may involve the caudal septum, anterior nasal spine, and the lower lateral cartilages.
• Midvault deviation consistently accompanies at least anterior and commonly mid and posterior septal deviation.
• In all types of septal deviation, the middle and/or inferior turbinates may be enlarged. The enlargement is usually juxtaposed to the concave side of the septum.
• There are six classes of septal deviation.
Technical steps
Nasal bones/upper lateral cartilage
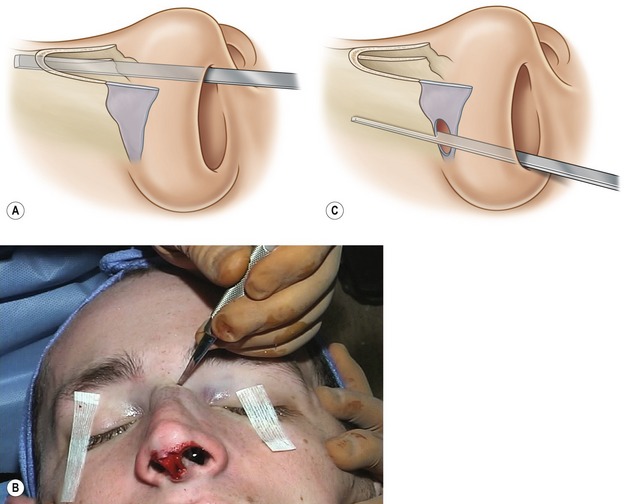
Prior to osteotomy, a push rasp is utilized in order to remove any bony hump. The rasp is angled toward the cheek to minimize the chance of septal fracture. After removing the hump, the upper nose is reassessed for symmetry. Often there may be far worse deviation than expected of the upper nose after hump removal. A medial osteotomy is first performed with a 4 or 6 mm osteotome, which is placed medial to the nasal bones and advanced cephalically with careful use of a mallet (Fig. 42.4A). A vertical osteotomy is then done with a 2 mm osteotome. The osteotome is percutaneously placed anteriorly in order to avoid the angular vessels (Fig. 42.4B). It is then directed posteriorly and cephalically and several interrupted osteotomies are made. After a small stab incision at the nasal vestibule with a #15 blade, a Joseph’s periosteal elevator is then used to incise the vestibular lining and elevate the periosteum. An internal low-to-low osteotomy is performed using a guarded osteotome and carried posterior to the natural suture line (Fig. 42.4C). A portion of the osteotomy is therefore made in the frontal process of the maxilla. This avoids the lateral step deformity seen after some osteotomies. Following adequate osteotomies, the upper lateral cartilages are assessed. There is often a discrepancy in the upper lateral cartilage length after the completion of the osteotomy. If a difference in length in the upper lateral cartilage exists, they may be trimmed in order to obtain symmetry. If the cephalic nasal asymmetry is unilateral only, the defect may be camouflaged using an onlay cartilage graft. However, correcting the unilateral defect with an osteotomy is preferred for its functional superiority.