Correction of Orbital Roof Fractures
Samita Sally Goyal
John N. Jensen
DEFINITION
Orbital roof fractures may occur in isolation but more often are a part of a larger pattern of traumatic injury.
Classification1:
Nondisplaced fractures
Isolated blow-in fractures
Orbital roof displaced inferiorly into orbit
No involvement of supraorbital rim or frontal sinus
Due to sudden increased intracranial pressure and shift of the cranium and intracranial contents; usually associated with severe brain injury
Leads to decreased volume of orbit and possible displacement of globe
Most likely injury type to require surgical intervention
Isolated blow-up (blow-out) fractures
Orbital roof displaced superiorly into anterior cranial fossa
No involvement of supraorbital rim
Due to increase in intraorbital pressure, hydraulic force, or shear strain
Leads to increased volume of orbit
Roof (blow up or blow in) fracture including supraorbital rim
ANATOMY
The orbital roof is thin, slightly concave bone that separates orbital contents and the anterior cranial fossa.
It may include the lateral extent of the floor of the frontal sinus
Consists primarily of the orbital plate of the frontal bone; lesser (posterior) contribution is from the greater and lesser wings of the sphenoid bone (FIG 1)
The endocranial surface is characterized by multiple ridges and thin bone that may have a role in fracture patterns.
The orbital surface is smooth and thin and includes the lacrimal fossa, a depression in the anterolateral orbital roof that contains the lacrimal gland.
The supraorbital rim confers rigidity to the superior orbit.
Structures in proximity to the orbital roof include the following:
Orbital septum
Lacrimal gland
Superior rectus muscle
Superior oblique muscle
Levator palpebrae superioris muscle
Supraorbital and supratrochlear nerves
Superior division of the oculomotor nerve
Globe
PATHOGENESIS
Orbital roof fractures make up 1% to 9% of all facial fractures.
Likely to have craniofacial, intracranial, ophthalmic, or other bodily injuries (isolated orbital roof fractures in adults are rare)
In adults, most commonly seen in men 20 to 40 years of age (89%-93%).2
More commonly seen in pediatric patients under 7 years of age3:
Children older than 7 years are more likely to sustain orbital floor fractures.
Young children have a high cranium:orbit ratio, incompletely pneumatized frontal sinus makes less likely shock absorption than in older children/adults; in high-energy impact situations, energy is more efficiently transmitted through the orbital roof.
Most commonly due to high-energy impact injuries to the face
Etiology
Motor vehicle crash (high energy): higher risk of comminution3
Fall: more likely linear pattern3
Assault
Commonly seen at the junction of middle and medial thirds of orbital roof
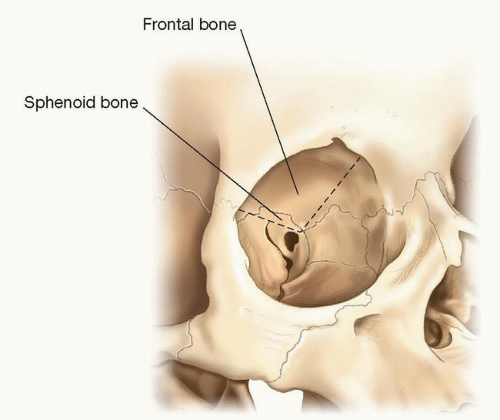
FIG 1 • Submental view of orbital skeletal anatomy demonstrating that the majority of the roof is frontal bone.
Concomitant facial fractures2:
Frontal sinus (95%)
Orbital rims (60%)
Naso-orbital-ethmoidal region (33%)
Orbital wall fractures (33%)
Le Fort fractures (27%)
Also associated with fractures of the cribriform plate, lateral orbital wall, squamous portion of the temporal bone, and planum sphenoidale
Concomitant soft tissue injuries: 25% of all fractures involving orbit have ocular injuries.4
NATURAL HISTORY
In pediatric fractures, orbital roof fractures may develop into growing fractures3:
Growing skull fractures—cranial fracture combined with dural tear and brain herniation in a growing brain—can lead to progression of osseous defect with growth.5
Frontal and parietal regions more commonly affected
More likely to be seen in children less than 3 years of age (period of rapid brain growth)
Suspect risk for development into growing fracture if imaging suggests herniation of intracranial contents into orbital region
Isolated orbital roof “blow-in” fractures may autoreduce with resolution of cerebral edema if the dura is reasonably intact and apposed to the bone.6
PATIENT HISTORY AND PHYSICAL FINDINGS
History
Blunt or penetrating facial trauma
Diplopia
Eye pain
Diminished visual acuity
Blindness
Physical findings
Superior orbital rim contour deformity
Periorbital or conjunctival ecchymosis and edema
Epiphora
Hypesthesia/paresthesia of supraorbital and/or supratrochlear nerves
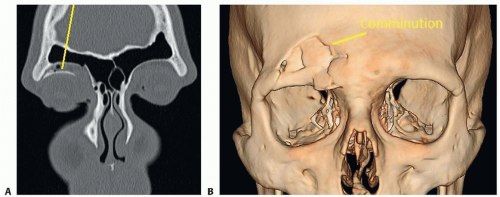
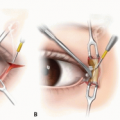
FIG 2 • Comminuted orbital roof/frontal sinus fracture with rim involvement in a 19-year-old following blunt force trauma (baseball). The patient had a ptotic upper lid secondary to inferior displacement of orbital roof (indicted by leader in (A)). B. 3D CT scan demonstrating the comminuted fracture.
Orbital emphysema
Soft tissue lacerations
Enophthalmos/hyperglobus (blow-out fracture)
Exophthalmos/hypoglobus/proptosis (blow-in fracture)
Extraocular muscle entrapment or imbalance (superior rectus muscle) with disconjugate gaze
Blepharoptosis due to injury to the levator palpebrae
Afferent pupillary defect
Neurological comorbidity
Dural injury with cerebrospinal fluid (CSF) leak (clear rhinorrhea)
Intracranial hemorrhage
Pneumocephalus (implies dural disruption)
Meningitis
Brain injury
Ophthalmic comorbidity
Optic nerve compression or laceration
Detached retina
Retrobulbar hematoma
Globe rupture
Ptosis or lagophthalmos
Intraorbital foreign bodies
Extraocular motor nerve palsies
Orbital encephalocele/intrusion
IMAGING
Standard of care imaging modality: thin-slice (1 mm) computed tomography (CT) scan1:
Axial, coronal, and sagittal views essential to provide complete assessment of degree of displacement and impact on surrounding structure.
3D views not essential, but can be helpful in badly displaced/comminuted fractures, especially if utilizing a limited access approach
Advantages: rapid, available, provides ability to assess intracranial content/injury
Magnetic resonance imaging (MRI): impractical as it is an insensitive exam of the bone and some foreign objects; contraindicated in situations where metallic foreign objects (bullet fragments) may be present in soft tissues (FIG 2).
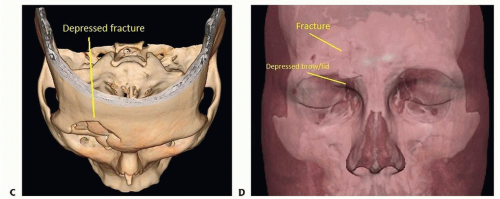 FIG 2 (Continued) • C. 3D CT bird’s eye view of the fracture. D. Soft tissue envelope demonstrating the depressed eyebrow associated with the fracture. |
NONOPERATIVE MANAGEMENT
Conservative, nonoperative management is often appropriate in orbital roof fractures and indicated in
Isolated, nondisplaced, or minimally displaced orbital roof fractures
Initial nonoperative course in “blow-in” fractures associated with intracerebral edema; observe for reduction of fracture fragment with resolution of cerebral edema6
Children without signs of functional deficit (eyelid position/function, extraocular muscle mobility) or significant displacement
Higher threshold to operate in children (more likely to tolerate conservative management) but certain fracture patterns may have potential for growing skull fractures (significant displacement with concomitant dural injury5).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree