Correction of Le Fort III Fractures
Joseph Lopez
Amir H. Dorafshar
DEFINITION
Le Fort III type fracture lines classically transverse the horizontal and vertical buttresses of the face, separating the face from the base of the skull.
Also known as craniofacial disjunction, Le Fort III type fracture lines extend specifically from the lateral and medial orbital walls to the nasofrontal region and the zygomatic arches (FIG 1).
ANATOMY
The facial skeleton is composed of several bones: maxilla, mandible, lacrimal, nasal, palatine, vomer, zygomatic, and inferior nasal concha bones.
The maxilla constitutes the middle third of the face and contains the maxillary sinus.
The maxilla and the surrounding bones compose an important system of buttresses that provide mechanical support to the face.
These buttresses include the lateral orbital wall, zygomatic arch, nasofrontal, and lateral and medial maxillary buttresses.
The medial and lateral maxillary buttresses are better known as the nasomaxillary buttress and zygomaticomaxillary (ZMC) buttress, respectively (FIG 2).
These buttresses (ie, nasofrontral, zygomatic arch, zygomaticofrontal, lateral orbital wall) are critical for bony alignment and stabilization after fractures.
The main fracture line of Le Fort III type fractures extends from the bridge of the nose through the nasofrontal process, the medial and lateral walls and floor of the orbits, the zygomaticofrontal processes, and the zygomatic arches.
The nasal septum is also fractured, and the maxilla is separated from the pterygoid plates.
The maxilla is highly vascularized. The largest branch of the external carotid artery, the internal maxillary artery, supplies the midface.
Sensation to the maxillary teeth, nasal cavity, sinuses, and facial skin overlying the maxilla is supplied by the second branch of the trigeminal nerve (infraorbital nerve).
The infraorbital foramen is located 5 to 10 mm below the infraorbital rim in line with the medial limbus of the pupil.
PATHOGENESIS
All maxillary fractures, including Le Fort III type, are a result of high-energy frontal or lateral impacts to the face.
When force is exerted on the maxilla and the surrounding bones, the force is dissipated in such a way that the globe and brain are protected from injury, resulting in characteristic fracture patterns.
Maxillary fractures are categorized using the Le Fort system.
Le Fort I and II type fractures are less complex maxillary fractures (and are not discussed here). Le Fort III type fractures are the most complex maxillary fractures and are often the result of high-energy facial injuries.
Le Fort III type fractures usually present in a mixed pattern with other Le Fort type fractures often present (eg, Le Fort I and II).
Le Fort III type fractures often present with other facial fractures such as mandible, ZMC, or naso-orbital-ethmoid (NOE) fractures.
Le Fort III type fractures are often also associated with cervical spine and skull base fractures. These fractures may be associated with airway compromise, facial bleeding, and neurological injuries.
PATIENT HISTORY AND PHYSICAL FINDINGS
All initial trauma evaluations should consist of an assessment of airway, breathing, and circulation (ie, A, B, Cs).
A proper primary and secondary survey should be performed in all patients with suspected facial trauma.
Because Le Fort III type fractures are the result of highenergy trauma, patients can often present with other life-threatening injuries such as intracranial bleeding or penetrating trauma.
After the patient is stabilized, a complete history should be obtained (often from a family member or witnesses given that Le Fort III type fractures are associated with neurological injuries or loss of consciousness). The following questions should be considered:
When and where did the accident occur?
What are the specifics of the injury (ie, object, speed, direction)?
Was there loss of consciousness?
Does the patient have the following symptoms:
Loss of vision?
Hearing changes?
Malocclusion?
Altered sensation?
Difficulty moving eyes?
Pain with jaw movement?
A complete review of system should be obtained including allergies, medications, previous surgeries or medical conditions, and tetanus immunization history.
A thorough history can be instrumental in guiding the CMF surgeon to specific injury patterns.
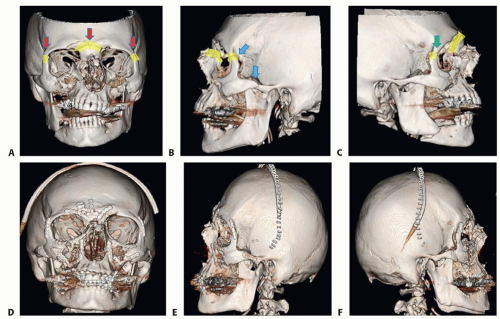
FIG 1 • Craniofacial disjunction/Le Fort III type fracture in a 28-year-old healthy male after a high-impact motor vehicle collision. A. Le Fort III type fractures are typified by fracture lines across the bilateral lateral orbital walls and nasofrontal junctions (red arrows). B. Left zygomatic arch and zygomaticofrontal suture fracture (blue arrows). C. Right zygomaticofrontal junction fracture (green arrow). D. Stabilization achieved by reduction and fixation of the nasofrontal junction, bilateral orbital walls, and zygomaticofrontal junctions. E,F. Fixation of bilateral zygomaticofrontal fractures.
Assess the head and neck region for the following:
Soft tissue asymmetry or skeletal deformities: Le Fort III patients often present with elongated faces or malar depression.
Ear canals and tympanic membrane for traumatic injuries (ie, hemotympanum, etc.) or CSF leaks
Nasal area for epistaxis, CSF rhinorrhea, swelling, septal deviation or hematoma, and nasal airway obstruction
Orbit for entrapment, ecchymosis, edema, or subconjunctival hemorrhage
Dentition for malocclusion, mobility of teeth, prosthetics, or mandibular/maxillary displacement during teeth contact: Le Fort III type fractures can present with malocclusion.
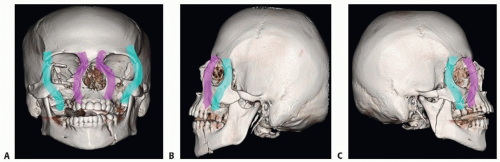
FIG 2 • 3D reconstructions created from CT maxillofacial coronal (A), axial (B), and sagittal (C) images of a 19-year-old healthy man with a Le Fort III type fracture pattern after falling 15 ft. The purple lines display the nasomaxillary buttresses, and the aqua lines display the zygomaticomaxillary buttresses.
Oral mucosa for swelling, lacerations, open fractures, or other pathology
Occlusion for overjet, overbite, or open bite
Neurovascular examination
Cranial nerves
Assess for paresthesia in the distribution of the infraorbital nerve.
Palpation of the head and neck region for:
Step-offs, crepitus, clicking, or popping of the midface, nasal, frontal, and mandibular regions
Swelling or tenderness along buttress lines
Instability of the midface or maxillary mobility
Stability of the canthal attachments
IMAGING
Patients suspected of having Le Fort III type or other maxillary fractures should undergo computed tomography (CT) to evaluate the fracture patterns and the need for treatment:
CT scans should be reviewed in the coronal, axial, and sagittal planes with particular attention to the buttresses to determine severity and types of fracture lines.
3D reconstructions can often be useful for teaching purposes and for virtual surgical planning (FIG 2).
SURGICAL MANAGEMENT
The two most important indications for surgical intervention of maxillary fractures are malocclusion and instability:
Given the complexity of Le Fort III type fractures, almost all Le Fort III type fractures present with malocclusion or instability that require surgical management.
Other relative indications for Le Fort III type surgical management include uncontrolled bleeding and airway stabilization:
Because Le Fort III type fractures are associated with extensive soft tissue injury and swelling, nasal and oral airflow can be compromised.
The main goal of operative management is to re-establish proper occlusion.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree