Correction of Le Fort II Fracture
Nataliya Biskup
John A. van Aalst
DEFINITION
Le Fort II is a midface fracture pattern that classically involves the critical vertical facial buttresses:
Nasofrontal
Zygomaticomaxillary
Pterygomaxillary (pathognomonic component of all Le Fort fractures)
ANATOMY
The fracture starts at the zygomaticomaxillary buttress, extends through the inferior orbital rim and orbital floor to the nasofrontal buttress, and then travels posteriorly to involve the pterygomaxillary junction (FIG 1).
The level of fracture across the nose is variable, ranging from as high as the nasofrontal suture to as low as the nasal cartilages.
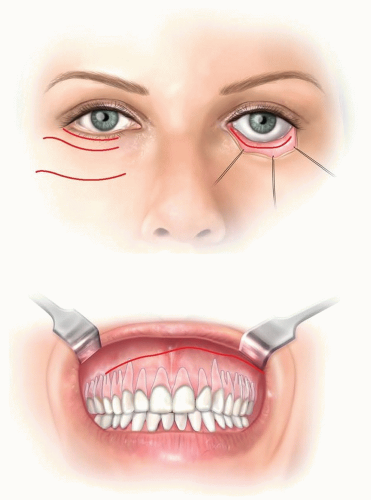
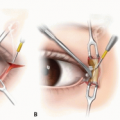
FIG 1 • Approaches for exposure of the maxilla for reduction and plating for Le Fort II fracture.
The attached pterygoid muscles exert a posterior and downward pull on the maxilla leading to an anterior open bite with class III occlusal relationship.
Fractures may be bilateral or unilateral, may be combined with other Le Fort fractures, and often may be a component of a pan-facial injury.
Medial and inferior orbital walls and nasoethmoid fractures are commonly associated fractures. If the fracture traverses the lacrimal fossa, it may involve the lacrimal system.
PATHOGENESIS
Le Fort II fractures result from high-velocity, blunt trauma, such as motor vehicle collisions.
Patients will often report being thrown forward striking the midface against an object such as a steering wheel.
PATIENT HISTORY AND PHYSICAL FINDINGS
In addition to diffuse facial edema, malocclusion, periorbital ecchymoses, and epistaxis are often present.
Mobility of the maxilla is a hallmark clinical finding.
Step-offs along the inferior orbital rim may be palpable.
The key points of examination are as follows:
Rule out cervical spine injury.
Evaluate ocular/orbital injury (vision, pupils, extraocular movement).
Assess cranial nerve V2 (sensation over cheek, lateral nose, and upper lip).
Evaluate occlusion. The expected occlusion is class III with an anterior open bite with premature posterior tooth contact.
IMAGING
Maxillofacial CT with 3D reconstruction is the standard for diagnosis and preoperative planning. Fluid in the maxillary sinus is the most reliable indicator of maxillary fractures.
EPIDEMIOLOGY
Most patients are males in their 30s involved in motor vehicle collisions.1
Among patients with maxillary fractures, the incidence of Le Fort I, Le Fort II, and Le Fort III fracture is 16% to 55%, 14% to 24%, and 13%, respectively.
Over half (57%) of the Le Fort fractures are combinations of the three; 89% coexist with other fractures in the maxillofacial region.2
The incidence of associated serious eye injury is 9% and traumatic optic neuropathy 20%, and the rate becomes significantly higher for more complex fractures.2,3
NONSURGICAL MANAGEMENT
Observation is indicated in:
Patients with nondisplaced fractures, premorbid, unchanged occlusion, and willingness to comply with strict soft, no-chew diet
Edentulous patients with minimal displacement
Unstable patients
Closed treatment with arch bars and guiding elastics is indicated in patients with minor malocclusion who can be reduced by closed maxillary disimpaction and manipulation.
SURGICAL MANAGEMENT
Open treatment is indicated in patients with displaced fractures or malocclusion or those unable to comply with diet modification.
Preoperative Planning
Rule out cervical spine injury prior to surgical correction of the facial fracture.
Obtain ophthalmologic evaluation to rule out globe/retinal injury as intraoperative manipulation may exacerbate the injury.
Positioning
Use nasotracheal intubation to facilitate verifying occlusion during fracture reduction.
If nasotracheal intubation is contraindicated, place the endotracheal tube through retromolar space; if this is not possible and other lacerations are present, use submental or submandibular intubation.6
Approach
Make an upper gingivobuccal sulcus incision from first premolar to first premolar, leaving a residual cuff of mucosa for final closure.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree