Reconstruction of the parotid defect is a complex topic that encompasses restoration of both facial form and function. The reconstructive surgeon must consider facial contour, avoidance of Frey syndrome, skin coverage, tumor surveillance, potential adjuvant therapy, and facial reanimation when addressing parotid defects. With each defect there are several options within the reconstructive ladder, creating controversies regarding optimal management. This article describes surgical approaches to reconstruction of parotid defects, highlighting areas of controversy.
Key points
- •
Multiple reconstructive options are available for parotidectomy defect reconstruction. These vary depending on the extent of parotidectomy—superficial, total, or radical.
- •
Reconstructive considerations include facial contour, avoidance of Frey syndrome, skin coverage, tumor surveillance, potential adjuvant therapy, and facial reanimation.
- •
Parotidectomy reconstruction should be tailored to the patient, specific to the defect, and within the comfort level of the reconstructive surgeon.
- •
Facial reanimation should be performed in radical parotidectomy reconstruction while giving consideration to patient age, comorbidities, prognosis, goals of treatment, and future adjuvant radiation therapy.
Introduction
Effective and aesthetically pleasing reconstruction of the parotidectomy defect requires full understanding of both facial form and function. To appropriately discuss the varying reconstructive methods available, defects created by superficial parotidectomy, total parotidectomy, and radical parotidectomy are addressed separately. Overall, reconstructive emphasis is placed on recreating facial contour, avoiding Frey syndrome, providing skin coverage, minimizing deleterious effects of adjuvant therapy, and restoring facial function. Areas of controversy are highlighted and discussed.
Introduction
Effective and aesthetically pleasing reconstruction of the parotidectomy defect requires full understanding of both facial form and function. To appropriately discuss the varying reconstructive methods available, defects created by superficial parotidectomy, total parotidectomy, and radical parotidectomy are addressed separately. Overall, reconstructive emphasis is placed on recreating facial contour, avoiding Frey syndrome, providing skin coverage, minimizing deleterious effects of adjuvant therapy, and restoring facial function. Areas of controversy are highlighted and discussed.
Superficial parotidectomy
Reconstruction of the superficial parotidectomy defect is usually easiest when performed primarily, because the defect and facial nerve are exposed. The greatest risk of secondary reconstruction is inadvertent facial nerve injury. Options for addressing facial asymmetry after superficial parotidectomy include abdominal fat grafting, use of injectable fillers, placement of acellular dermal matrix (ADM), sternocleidomastoid rotational flap, temporoparietal fascia (TPF) rotational flap, and superficial muscular aponeurotic system (SMAS) advancement flaps.
Although usually of minor significance, the contour defect after superficial parotidectomy can be disfiguring. In addition to facial asymmetry, Frey syndrome, also known as gustatory sweating, commonly affects patients undergoing superficial parotidectomy and is caused by aberrant reinervation of severed parasympathetic fibers to sweat glands of elevated cheek skin. The incidence of Frey syndrome ranges from 38% to 86% depending on if subjective or objective measures are used.
Frey syndrome can be treated secondarily with botulinum toxin type A; however, the therapeutic effect after injection with botulinum toxin type A is temporary and patients most affected by Frey syndrome may require lifelong recurrent injections. Secondary surgical procedures offering potential permanent solutions for Frey syndrome may place the exposed facial nerve at risk. Measures taken at the time of primary surgical treatment of the parotid to prevent the development of Frey syndrome provide optimal results. Several surgical techniques may be used, all of which involve placement of a barrier between remaining parotid tissue and the elevated skin flap. As an added benefit, this barrier can provide varying degrees of volume to the defect site to improve facial contour. Barrier options include abdominal fat, ADM, and autogenous vascularized tissue, such as sternocleidomastoid rotational flap, TPF rotational flap, and SMAS advancement flaps. There is some debate regarding the success rates of each technique (discussed later).
Abdominal Fat Grafting
Autologous fat transfer is a widely used technique for moderate contour defect restoration that has the benefits of simplicity, minimal donor site morbidity, and little additional operative time. Abdominal fat is typically harvested via a lower abdominal incision, and placed into the defect site en bloc ( Fig. 1 ). High patient satisfaction, correction of contour defect, and avoidance of Frey syndrome have been demonstrated in patients undergoing superficial or total parotidectomy with single-stage en bloc abdominal fat grafting.
A composite of de-epithelialized dermis with an en bloc fat graft, known as a dermofat graft, may likewise be applied to the parotid defect site. It is thought that inclusion of the dermis prevents fat necrosis and minimizes graft resorption. Dermofat grafts require larger harvest incisions, typically positioned at the lower abdomen, and subsequent de-epithelization. Results have shown that this technique is associated with little associated morbidity or additional operative time. Nosan and colleagues reported only 11% facial concavity after 4.5 years of follow-up using a dermofat graft to correct superficial parotid defects. Patients were overcorrected by 10% to 15% to account for resorption.
Curry and colleagues described a method of SMAS plication and dermofat grafting with a 10% to 20% overcorrection after superficial parotidectomy. This method resulted in a statistically significant decrease in facial asymmetry and symptomatic Frey syndrome in 34 patients. SMAS elevation is not always possible, however, after parotidectomy for malignancy.
Regardless of method, most investigators recommend initial volume overcorrection by 10% to 20% for optimal results. Preoperative or postoperative radiation therapy may increase fat reabsorption rate.
Some investigators suggest only performing fat grafting for benign parotid disease, such that the fat grafting does not interfere with tumor surveillance in malignant cases. Abdominal fat grafting after resection of parotid malignancy, however, has not been shown detrimental to clinical or radiologic tumor surveillance. Due to improved imaging techniques and the potential for recurrent tumors to spread deep or longitudinally, radiographic tumor surveillance offers many advantages to clinical evaluation in the monitoring of postparotidectomy patients. The distinctive appearance of fat on MRI allows for easy delineation of the fat graft from normal or pathologic parotid tissue.
Injectable Fillers
Although preferred, volume restoration of the superficial parotid defect may not always be performed primarily. Therefore, techniques for secondary volume restoration may be required. One method of secondary correction is with injectable synthetic dermal fillers to add volume to a concave region. Synthetic dermal fillers are widely used for facial volume loss related to ageing but can also be a beneficial method for patients with postoperative volume deformities. Two dermal fillers, poly- l -lactic acid and calcium hydroxyapatite, bear specific indication by the US Food and Drug Administration for treatment of HIV-associated lipoatrophy in the parotid region, but none has a specific indication for facial asymmetry after parotidectomy.
Poly- l -lactic acid is a biocompatible synthetic polymer that provides volume and incites a local tissue reaction to stimulate proliferation of fibroblasts. It is immunologically inert, safe, and well tolerated. Because of reabsorption over time, the volume correction lasts up to 2 years and a series of several injections is required for optimal results. Partially cross-linked hyaluronic acid dermal fillers are also used for management of facial volume loss in patients suffering from highly active antiretroviral therapy–related lipoatrophy and may also be used for secondary correction of facial asymmetry after superficial parotidectomy.
Acellular Dermal Matrix Placement
AlloDerm (LifeCell, Bridgewater, New Jersey) is one of several acellular matrix grafts derived from human cadaveric dermis that may be used for volume reconstruction of the superficial parotidectomy defect. Advantages of AlloDerm use include the lack of donor site morbidity and minimal additional operative time. AlloDerm is an allograft, however, and is limited by its risk for infection, extrusion, limited volume, and resorption. Govindaraj and colleagues prospectively studied AlloDerm placement compared with controls without any reconstruction and found the objective incidence of Frey syndrome was reduced to 0% in the AlloDerm group compared with 40% for the control group. There was a significantly higher incidence of seromas in the AlloDerm group, however, when compared with the control group (25% vs 9%, respectively). In this study, there was only 1 infection requiring removal of the graft in 32 patients. Sinha and colleagues also found successful reduction of subjective Frey syndrome with AlloDerm placement after superficial parotidectomy. Contrary to the previous study, there were no infections and no increase in seroma rates in the Alloderm group. A meta-analysis by Zeng and colleagues reviewed 5 randomized controlled trials evaluating the use AlloDerm for parotidectomy reconstruction and found an 85% relative risk reduction in objective Frey syndrome without any increase in wound infections or seromas with AlloDerm use compared with controls.
For volume reconstruction with AlloDerm, several pieces are folded to appropriate thickness and carefully secured into position to fill the superficial parotidectomy defect ( Fig. 2 ). Overall, this ADM reconstruction is limited by its potential for infection and resorption, variable added complexity during possible future reoperation, and added cost.
Local Muscle or Facial Rotational Flaps
Sternocleidomastoid rotational flap
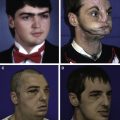
Transposition of the sternocleidomastoid muscle (SCM) to fill the parotidectomy defect was originally described by Jost and colleagues in 1968. The SCM flap can be superiorly or inferiorly based. For a superiorly based flap, the SCM muscle is split into 2 halves along the septum. Then a horizontal incision is used to free the anterior sternal insertion of the SCM muscle. Below this dissection, the accessory spinal nerve is isolated and protected. Finally, the muscle with its cervical fascia is rotated superiorly to fill the defect and sutured to the parotidomasseteric fascia ( Fig. 3 ). Inferiorly based flaps are incised at their most superior insertion into the mastoid tip and are mobilized anterosuperiorly into the parotid defect and are anchored to the zygomatic arch and masseter muscle.
The role of the SCM flap in prevention of Frey syndrome and in facial volume reconstruction after superficial or total parotidectomy has been controversial. Kornblut and colleagues found little benefit of the SCM flap in preventing Frey syndrome or facial asymmetry. Casler and Conley compared the SCM flap with SMAS plication and found both methods significantly reduced the incidence of Frey syndrome compared with controls, but there was a trend for better results with SMAS plication. Fasolis and colleagues directly compared SCM flap reconstruction to abdominal fat grafting and found improved cosmetic results with abdominal fat grafting. In this study, 5 of 11 patients receiving SCM flap reconstruction were unhappy with their facial or neck contour defect compared with 3 of 40 patients with abdominal fat grafting. A 2002 prospective randomized controlled trial by Kerawala and colleagues in 2002 found no advantage in patient-perceived or provider-perceived cosmetic outcomes or in the incidence of Frey syndrome in patients reconstructed with an SCM flap compared with controls without any reconstruction. Additionally, there was an increase in facial nerve weakness in the SCM group.
The SCM flap can pose an attractive option because it does not require any additional incisions or significant additional operative time. Due to proximity, however, it is associated with potential injury to the facial, spinal accessory, and greater auricular nerves. Furthermore, because it requires a portion of the SCM, it paradoxically creates a nearby cosmetic deformity with hollowing of neck, resulting in an exchange of one soft tissue concavity for another.
Temporoparietal fascia rotational flap
The TPF rotational flap has been described to reconstruct the parotid defect. To increase strength and bulk of the otherwise thin TPF flap, it can be elevated with the underlying deep temporalis fascia as a double-layered fascial flap. Ahmed and Kolhe evaluated 24 patients treated with a double-layered TPF flap and found it reduced Frey syndrome to 8% from 43% in controls and all patients had less noticeable contour defects. The benefits of the TPF flap are its thinness and pliability, good vascularity, and inconspicuous donor site ( Fig. 4 ). Damage to the superficial temporal vessels during the parotidectomy, however, limits viability of the flap. Further complications include alopecia, injury to the frontal branch of facial nerve, hematoma, and scar extension in the temporal region. Studies have shown success in avoiding Frey syndrome, although due to the thin nature of the flap, less than optimal cosmetic results are obtained while bearing increased operative time.