This article outlines current concepts in aging brows and lids, and focuses on the current “evolution” to the 3-dimensional construct. Relevant anatomy is reviewed in detail because thoughtful analysis of the underlying anatomy, ethnicity, gender, and goals of each patient will greatly enhance our ability to address site-specific corrections to achieve optimal and natural-looking results.
Key points
- •
Aging is a 3-dimensional process, with changes in multiple tissues contributing to the overall effect.
- •
Patients most commonly correlate aging changes with expressions of anger, sadness, and fatigue.
- •
The role of volume loss in the clinical changes observed in the aging face is becoming widely appreciated. Mastery of volume replacement has become essential to the successful practice of esthetic medicine.
- •
Lifting techniques alone, without addressing volume loss, can no longer adequately address the aging process in the upper third of the face. In fact, this approach may actually exacerbate, rather than ameliorate, the aging process.
- •
Rejuvenation of the eyelids and eyebrows requires an understanding of the interrelationships between these and other facial structures to ensure optimal outcomes.
- •
Anatomy informs concepts, concepts inform technique, and technique determines outcomes.
Introduction
Current literature suggests that the aging process is occurring in all tissue structures of the face and that a change in one area may greatly influence the neighboring tissues, leading to a cascade of secondary events. The central role of volume loss and deflation in the aging face, rather than ptosis alone, has been clearly illustrated by Lambros in a longitudinal photographic analysis of more than 100 patients spanning an average period of 25 years. These studies have eloquently demonstrated that volume loss in fact mimics gravitational descent.
The age-related changes in the eyelid and eyebrow continuum, similar to other regions of the face, should be thought of as a 3-dimensional construct with deflation rather than ptosis being the primary factor in the aging process. Esthetic facial rejuvenation has traditionally focused on surgical procedures, which are based on a paradigm of removing and lifting “excess” tissues to counteract gravitational changes. Open and endoscopic browlifting techniques, as well as “nonsurgical” eyebrow lift with chemodenervation, have been widely used in clinical practice. Approaching the aging face from the standpoint of volume loss invokes an entirely different paradigm of rejuvenation. Instead of simply excising and lifting the tissues, the volume paradigm invokes the concept of “filling” the face. The focus of this article, outlining current concepts in the aging brows and lids, therefore focuses on this current “evolution” to the 3-dimensional construct. Although we often look for ideals, such as the perfect cheek, perfect lip, or perfect brow position, there is likely no singular esthetic that fits every individual face. Thoughtful analysis of the underlying anatomy, ethnicity, gender, and goals of each patient will greatly enhance our ability to address site-specific corrections to achieve optimal and natural-looking results. For this reason, relevant anatomy is reviewed in detail here.
Introduction
Current literature suggests that the aging process is occurring in all tissue structures of the face and that a change in one area may greatly influence the neighboring tissues, leading to a cascade of secondary events. The central role of volume loss and deflation in the aging face, rather than ptosis alone, has been clearly illustrated by Lambros in a longitudinal photographic analysis of more than 100 patients spanning an average period of 25 years. These studies have eloquently demonstrated that volume loss in fact mimics gravitational descent.
The age-related changes in the eyelid and eyebrow continuum, similar to other regions of the face, should be thought of as a 3-dimensional construct with deflation rather than ptosis being the primary factor in the aging process. Esthetic facial rejuvenation has traditionally focused on surgical procedures, which are based on a paradigm of removing and lifting “excess” tissues to counteract gravitational changes. Open and endoscopic browlifting techniques, as well as “nonsurgical” eyebrow lift with chemodenervation, have been widely used in clinical practice. Approaching the aging face from the standpoint of volume loss invokes an entirely different paradigm of rejuvenation. Instead of simply excising and lifting the tissues, the volume paradigm invokes the concept of “filling” the face. The focus of this article, outlining current concepts in the aging brows and lids, therefore focuses on this current “evolution” to the 3-dimensional construct. Although we often look for ideals, such as the perfect cheek, perfect lip, or perfect brow position, there is likely no singular esthetic that fits every individual face. Thoughtful analysis of the underlying anatomy, ethnicity, gender, and goals of each patient will greatly enhance our ability to address site-specific corrections to achieve optimal and natural-looking results. For this reason, relevant anatomy is reviewed in detail here.
Youthful and aging brows and lids
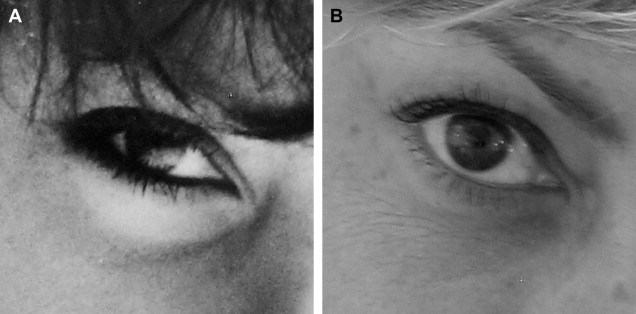
In youth, the 3-dimensional surface contours of the face predominantly reflect light. Volume changes over time result in broken reflections with intervening shadows. This is beautifully illustrated in Fig. 1 , which shows 2 pictures of the same woman, one from her high school years and the other 37 years later. The profound global volume loss in the older photograph is easy to appreciate. The youthful oval face in the frontal view dramatically flattens with age. The young eye appears long and full, the bony orbit is not visible, the skin is elastic and thick, most of the upper lid is concealed by the full brow, with only a few millimeters of upper lid show. The upper lid sulcus lacks a shadow, and the eye has an overall “almond” configuration, with the lid margin, lid crease, and eyebrow all parallel.
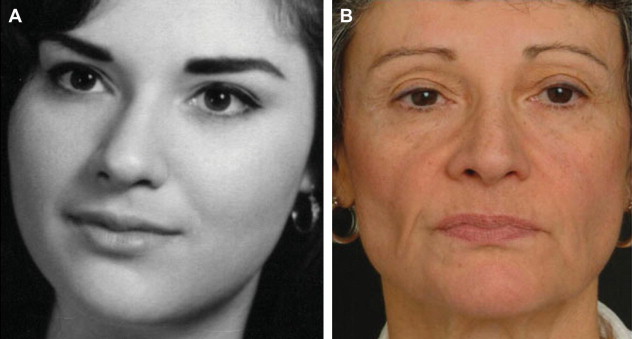
All of these characteristics are affected by aging in predictable ways. In the older photograph, we see brow deflation that does not result in significant brow ptosis, but rather results in the brow laying flat against the orbital rim. Shadows develop below the brow and in the concave temple. As the upper lid deflates, a fold of skin develops where there was once fullness, and the shadow of the upper lid sulcus emerges. With increasing age, this fold of upper lid skin often droops and may encroach on the lash line, completely effacing any visibility of the upper lid (“hooding”). The eyelid skin may also slip into the lid crease, revealing the upper lid veiled in youth by the full brow. Often this is initially most pronounced medially resulting in the so-called “A-frame” deformity.
More than 20 years ago, Van den Bosch and colleagues collected and analyzed data on eyeball and eyelid position of 320 men and women, equally divided into 10-year age cohorts between the ages of 10 and 89 years, and found that aging mainly affects the size of the horizontal eyelid fissure, which lengthens by about 10% between the ages of 12 and 25, and then shortens by almost the same amount between middle age and old age. Additional findings from their study were a higher skin fold (meaning increased upper lid show), and higher eyebrow position in both sexes. Sagging of the lower eyelid was noted, especially in men. These changes seen with aging (an increased upper lid show, which makes the eye look taller vertically, in combination with a horizontal shortening) result in a perceived “rounding” of the eye.
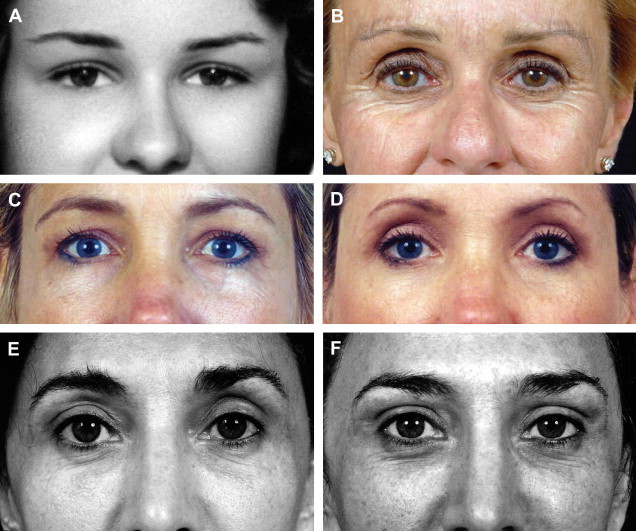
These changes are extremely well illustrated in Fig. 2 , taken from Lambros’ article on volumizing the brows. The top pair of pictures of the same woman at 21 and 64 years old demonstrate how the eyes have an almost “almond”-shaped appearance in youth and a more rounded configuration with aging. In the middle row, a photograph of a 45-year-old woman before and after blepharoplasty illustrates that conventional excisional techniques involving removal of “excess” skin and fat may actually exacerbate the hollowing of the orbit, with the subsequent appearance of a rounder shortened eye (ie, an older-appearing eye). Finally, on the bottom row, we see an older woman with rounded eyes. As the upper lid deflates, a fold of skin develops where there once was fullness, and the shadow of the upper lid sulcus emerges (especially on her right). Volumizing the upper brow with local anesthesia in this patient results in a less-rounded, more almond-shaped eye, resulting in a more youthful-appearing periorbital area.
Aging of the upper third of the face, of course, affects much more than esthetics. The eyes and the periorbital structures convey a wide range of expressions, representing a critical nonverbal form of communication that is fundamental to all of our social interactions. The basic expressions of happiness, sadness, fear, anger, and surprise appear to cross cultural lines and may be considered a universal means of nonverbal communication. Facial interpretation is in fact considered to be among the most important acquisitions in our development. Some forms of facial expressions, such as anger (glabellar furrows), sadness (downward angulation of the oral commissure), and fatigue (tear trough deformity), may be mimicked by the aging process. This generally leads to an unintended and undesirable misinterpretation of mood by others that is unwelcome to most all of us as we age and is one of the most common presenting complaints ( Fig. 3 ).

In a study in 2008, Knoll and colleagues had a set of images adjusted to only one variable reviewed by subjects and graded for of each of 7 expressions/emotions as follows: “surprise,” “anger,” “sadness,” “disgust,” “fear,” “happiness,” and “tiredness.” They found statistically significant values for tiredness were achieved by changes of increasing and decreasing the pretarsal skin crease (to simulate a long upper lid show or “hooding” with no lid show) and by depressing the lateral brow. Elevation of the medial brow elicited a minimal increase for sadness. All of these changes may also be seen with aging. Interestingly, simulating the skin resection of an upper blepharoplasty resulted in an increase in the perception of tiredness, perhaps indicating that skin excision without regard to volume may exacerbate, rather than ameliorate, the appearance of aging.
Relevant anatomy
Skin
Over the past decade, substantial progress has been made toward understanding the underlying mechanisms of the aging process. A major feature of aged skin is fragmentation of the dermal collagen matrix that leads to the loss of structural integrity and impairment of fibroblast function. Fragmentation results from actions of specific enzymes (matrix metalloproteinases) observed in both intrinsic and extrinsic aging. Fibroblasts that produce and organize the collagen matrix cannot attach to fragmented collagen and subsequently collapse. Collapsed fibroblasts produce low levels of collagen and high levels of collagen-degrading enzymes. Once a critical amount of collagen has been lost, this imbalance advances the aging process in a self-perpetuating, never-ending deleterious cycle. This is well illustrated by the difference in skin elasticity seen on the driver’s side and non–driver’s side window of the truck driver pictured in Fig. 4 . The production of new collagen demonstrated by electron microscopy after the injection of hyaluronic acid is felt likely to be attributable to a mechanical stretch effect, serving to rebalance collagen production and degradation, and thereby slowing its loss.

Bone
Craniofacial bony remodeling is increasingly being recognized as an important contributor to the facial aging process. More than a decade ago, Pessa and Chen studied 30 male skulls in 3 age categories at the Smithsonian Institution and found that although there was no change in width or height of the orbit with increasing age, there was curve distortion of the superomedial and inferolateral orbit. They also noted that this change in shape as well as size reflected a selective pattern of resorption and renewal occurring with age.
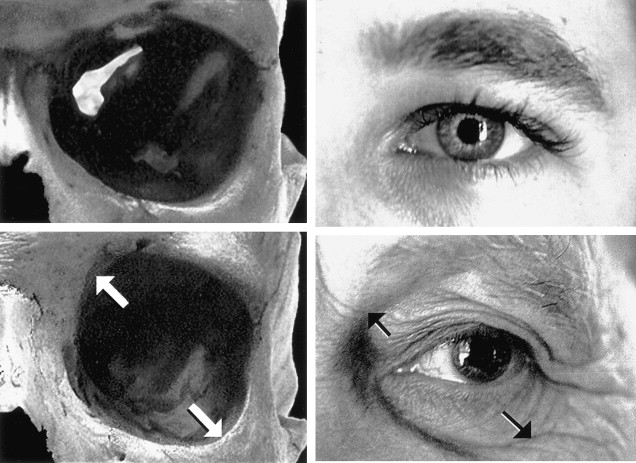
Subsequently, drawing on the common observation that a change in the underlying bony support from facial trauma could lead to changes in the draping of the soft tissues of the face, Pessa then hypothesized a corollary: it was logical that changes in the bony orbit could also be associated with changes in the overlying soft tissue. Specifically, that the redraping of soft tissue overlying the remodeled bony orbit may contribute to the development of a lateral suborbital tear trough and increased scleral show ( Figs. 5 and 6 ). Multiple studies have now demonstrated these craniofacial skeletal changes with age, most notably the landmark study by Shaw and Kahn.
Soft Tissue (Muscle and Fat)
Muscle dynamics play a central role in the changes seen in the aging forehead and brow.
Ellis and Masri studied 60 patients, age 20 to 74 years, who they split into 3 groups according to the dominant animation pattern: brow lifters, frowners, and squinters. They found that brow ptosis was accentuated laterally in the squinters and medially in the frowners, and that the brow lifter group showed more uniform displacement of the eyebrows. Animation patterns acquired in childhood, therefore, may have a significant effect on patterns of brow ptosis.
What happens to muscles with aging is likely contingent on a number of variables. Traditional thought holds that muscles become more lax with time. Some researchers now believe the muscles of facial animation may adjust to shifts in underlying volume by adjusting (and increasing) their resting tone. This may have clinical relevance regarding the depth at which we choose to place our fillers, as there may be some advantage to deeper placement.
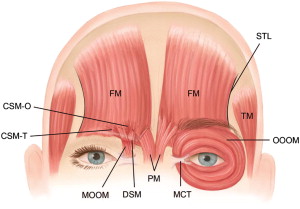
The medial brow depressors are made up of the centrally located procerus, surrounded laterally by 2 pairs of muscles: the corrugator supercilli and the depressor supercilli. The procerus is often a bifid muscle. It originates over the nasal dorsum, inserts into the skin of the glabella, and contributes to the horizontal lines over the nasal dorsum. The corrugator supercilii is the largest of the depressor muscles. It has both a transverse and a medial head with an origin at the medial orbital bone and an insertion on the underside of the frontalis muscle over the midbrow. The corrugator pulls in and down, contributing to the formation of the vertical glabellar rhytides, commonly referred to as “the elevens.” The depressor supercilii is a small muscle relative to the other depressors and runs almost vertically between the medial orbital bone and the medial head of the brow ( Fig. 7 ).
The orbicularis oculi muscle is a concentric muscle originating at the medial orbital bone and consists of 3 parts:
- 1.
Pretarsal: starting at the lid margin
- 2.
Preseptal: between the distal edge of the tarsal plate and the orbital rim
- 3.
Preorbicularis: covering the bony orbit distal to the rim
The medial portion of the orbicularis oculi is also a depressor of the medial brow. The lateral orbicularis oculi is a lateral brow depressor (which contributes to the formation of crow’s feet).
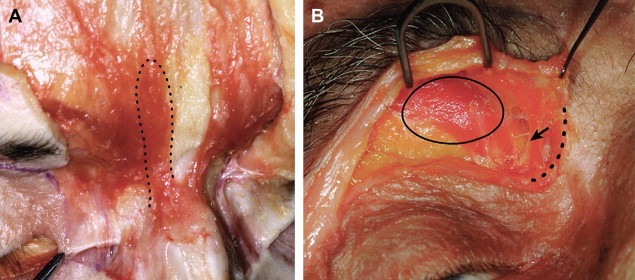
The elevator of the brow is the frontalis muscle. It is also most often found as a bifid muscle in which the right and left halves do not usually meet in the middle of the forehead ( Fig. 8 ). Using cadaveric dissections, Knize noted that the lateral margin of frontalis muscle almost always ends or becomes markedly attenuated along or just lateral to the temporal fusion line of the skull and its continuation as the superior temporal line. Among cadaver specimens, the temporal line was found to intersect the eyebrow at variable points ranging from the middle third of the eyebrow to just lateral to the eyebrow. The more medially that the plane of the temporal line meets the eyebrow, the less frontalis muscle resting tone there is for suspensory support for the lateral eyebrow. Among different patients, then, the ability of the frontalis muscle to maintain lateral eyebrow position may be variable. Additionally, the presence of a lateral orbital retaining ligament between the superficial temporal fascia and the zygomaticofrontal suture fixes the lateral eyebrow, preventing movement to a degree equivalent to the medial brow. Additionally, Knize notes that the preseptal fat pad and galea fat pad may facilitate gravitational descent of the unsupported overlying lateral eyebrow ( Fig. 9 ). The photos to the right of the schematic were chosen to illustrate how this may appear clinically. Details on medial brow anatomy are outlined in the schematic seen in Fig. 10 and cadaveric dissections of this region are seen in Figs. 11 and 12 .