Introduction
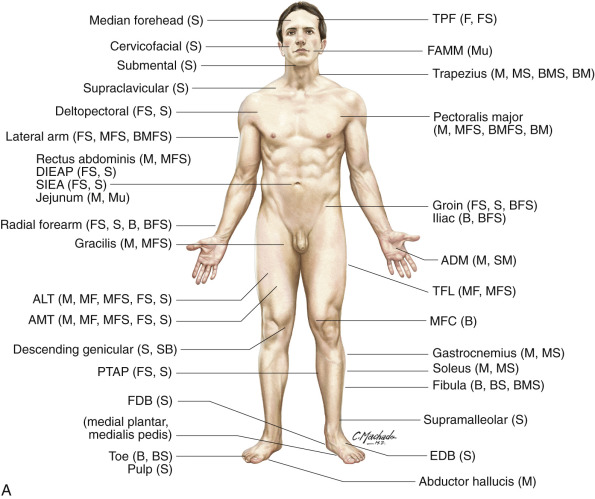
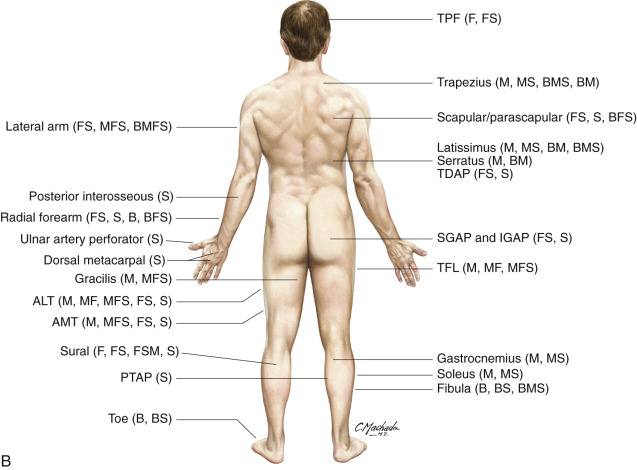
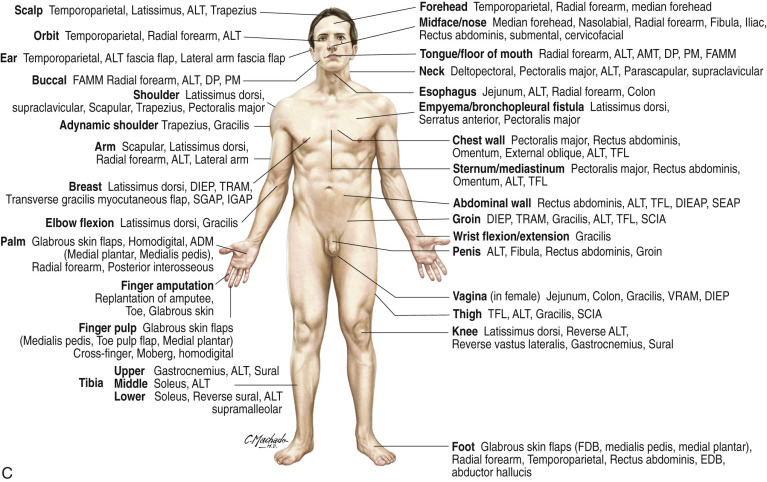
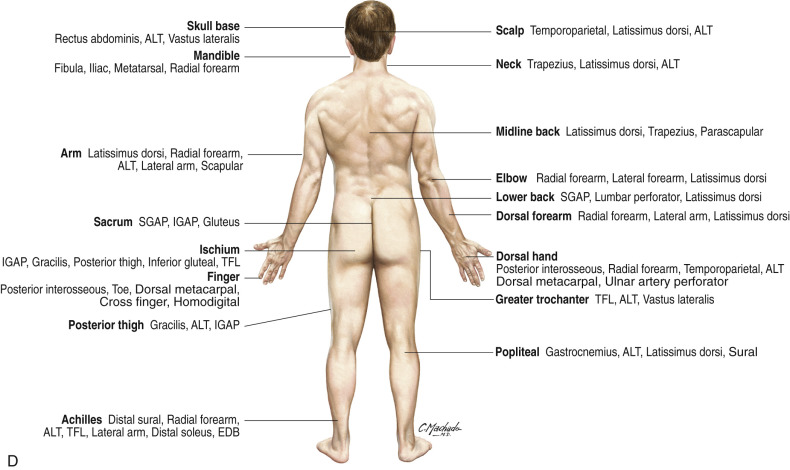
A meticulous preoperative problem analysis leading to the selection of the proper strategy for solving the given wound, defect, or deformity can be a difficult task, yet certainly as critical as the actual surgical procedure that may be required. If a vascularized tissue transfer is indicated, there can then be little question that the selection of the correct flap is imperative as, if chosen improperly, the entire reconstructive endeavor may be doomed to failure – no matter how careful the subsequent surgical execution. This initial phase of planning should be appreciated as the most intellectually stimulating and challenging stage, as sometimes the hours spent in the operating room afterwards may seem actually too much like “work.” Unfortunately, if simplicity were the only goal, unlike the early days of plastic surgery, when the only option was to use some variation of the random flap, now an almost overwhelming cornucopia of flap alternatives is available. A “laundry list” of all the available flaps and their indications would be an impossible job, even if limited to the “workhorse” flaps outlined in the other chapters in this book ( Fig. 3.1 ); but a brief dissertation on basic principles to follow in completing this selection process may prove invaluable. An appreciation of the attributes and limitations of the many available flaps ( Tables 3.1–3.6 ) and their specific indications for use ( Tables 3.7–3.9 ) is critical before a decision can be made as to which is most appropriate for the task at hand.
| Colon | Glabrous skin | Jejunum | Joints | Nail beds | Toe | |
|---|---|---|---|---|---|---|
| Ease of dissection | Simple | Not easy | Easy | Moderate | Difficult | Moderate |
| Anatomic anomalies | No | Usually | No | Common | No | Common |
| Potential for harvest as compound flap/component tissues that can be included | No | No | No | Yes/bone, skin | Yes/any part of toe | Yes/any part of foot |
| Contour (thin → bulky) | Bulky | Thin | Moderate thickness | N/A | N/A | N/A |
| Implant osseointegration | N/A | N/A | N/A | No | N/A | Yes |
| Donor site morbidity | Laparotomy needed | Minimal | Laparotomy needed | Can be minimal | Loss of nail | First toe, yes; Second toe, minimal |
| Bone length | N/A | N/A | N/A | Shorter | Variable | Short |
| Vascular pedicle caliber | Large | Small | Very large | Large | Small | Large |
| Vascular pedicle length | Long | Short | Very long | Medium | Short | Medium |
| When used as pedicled flap | ||||||
| Arc of rotation | Wide | Limited | Moderate | N/A | N/A | N/A |
| Reliability | Good | Moderate | Good | N/A | N/A | N/A |
| Potential for harvest as distally based | N/A | Yes | N/A | N/A | N/A | N/A |
| Flap | Free microvascular transfer | Pedicled | ||
|---|---|---|---|---|
| Typical indication | Atypical indications | Typical indication | Atypical indications | |
| Temporoparietal fascia | Thin, gliding surface to cover tendons, especially hand | Hair transplant | Ear salvage | Beard or eyebrow reconstruction |
| Pectoralis major | None | None | Closure of chest or facial wounds | Repair of esophagus or trachea |
| Deltopectoral | None | None | Oropharynx | Chest wounds |
| Rectus abdominis | Breast reconstruction | Lower extremity | Breast reconstruction | Groin |
| Jejunum | Cervical esophagus | Oropharynx lining | N/A | N/A |
| Trapezius | None | None | Midline posterior neck coverage | Lateral face |
| Scapular and parascapular | Large defects | Bone flap | Axillary contractures | Head and neck coverage |
| Latissimus flap | Large defects | Quadriceps function restoration | Breast, chest wounds, thoracic spine | Axillary contractures, head and neck, dynamic upper extremity |
| Flap | Free microvascular transfer | Pedicled | ||
|---|---|---|---|---|
| Typical indication | Atypical indications | Typical indication | Atypical indications | |
| Lateral arm | Small defect of arm or leg | Short segment bone or tendon defect | Elbow coverage | Axilla |
| Radial forearm | Oral lining | Foot or distal third leg | Hand coverage | Elbow coverage |
| Iliac | Mandible | Long bone segmental defects | Pubis | Sacrum |
| Groin | Large defect if cosmetic donor site imperative | Extremities | Thigh or abdomen | Staged upper extremity pedicle flaps |
| Gluteus | Breast reconstruction | None | Sacral or ischial pressure sores | Lumbar pressure sores |
| Tensor fascia lata | Vascularized fascia, Achilles repair | Abdominal wall | Abdominal wall | Groin |
| Gracilis | Small extremity wound, facial reanimation | Breast reconstruction | Groin, perineum or vagina | Scrotum, penis |
| Gastrocnemius | None | Pressure sore | Knee wound | Cross-leg flap |
| Soleus | None | None | Proximal leg | Distal leg |
| Fibula | Mandible or large bone segmental gap | Pelvis | Knee arthrodesis | Ipsilateral tibia segmental gap |
| Glabrous skin | Hand | Foot | Foot | None |
| Toe | Hand | Nail transfer | N/A | N/A |
| Flap | Free microvascular transfer | Pedicled | ||
|---|---|---|---|---|
| Typical indication | Atypical indications | Typical indication | Atypical indications | |
| Deep inferior epigastric artery perforator flap | Breast reconstruction | Large soft tissue defect | Groin coverage | Abdomen |
| Superficial inferior epigastric artery perforator flap | Breast reconstruction | Extremity defect | Groin | Staged upper extremity coverage |
| Superior gluteal artery perforator flap | Breast reconstruction | None | Sacral pressure sores | Lumbar pressure sores |
| Inferior gluteal artery perforator flap | Breast reconstruction | None | Ischial pressure sores | Perineum |
| Anterolateral thigh (ALT) flap | Large soft tissue defect | Achilles tendon | Thigh wounds | Abdomen |
| Anteromedial thigh flap | Large soft tissue defect if ALT flap unavailable | None | Thigh wounds | Groin |
| Thoracodorsal artery perforator flap | Large soft tissue defects | Breast reconstruction | Breast reconstruction | Axilla |
| Posterior tibial artery perforator flap | Thin contour required | None | Distal lower extremity | None |
| Bone | Cutaneous non-perforator based | Cutaneous perforator | Intestine | Muscle | Toe | |
|---|---|---|---|---|---|---|
| Ease of dissection | Somewhat difficult | Easy | Difficult | Requires laparotomy | Easy | Moderately difficult |
| Anatomic anomalies | Occasional | Rarely important | Expected | Rare | Rare | Common |
| Availability | Always | Always | Usually | Always | Always | Possible |
| Potential for harvest as compound flap | Sometimes | Sometimes | Always | Never | Usually | Sometimes |
| Contour (thin → bulky) | N/A | Variable | Variable | Moderate thickness | Relatively thin | N/A |
| Potential for thinning | No | Secondarily | Immediate | No | Yes | No |
| Donor site morbidity | Potential | If skin graft necessary | If skin graft necessary | Requires laparotomy | Loss of function | Potential, especially great toe |
| Dynamic transfer | No | No | No | No | Yes | No |
| Expendability | Maybe | Yes | Yes | Yes | Maybe | Maybe |
| Reliability (blood supply) | Usually good | Can be precarious | Usually good | Always | Best | Sometimes |
| Sensibility | No | Yes | Yes | No | No | Yes |
| Surface area | N/A | Small | Very large | Moderate | Large | N/A |
| Vascular pedicle caliber | Large | Variable | Can be large | Very large | Large | Large |
| Vascular pedicle length | Short | Variable | Exceedingly long | Very long | Medium | Medium |
| When used as pedicled flap | ||||||
| Arc of rotation | Short | Limited | Wide | N/A | Wide | N/A |
| Reliability | Usually good | Can be precarious | Usually good | N/A | Best | N/A |
| Need for supercharge | Sometimes | Usually not possible | Sometimes | N/A | Not possible | N/A |
| Gracilis | Gastrocnemius | Gluteus | Latissimus dorsi | Pectoralis major | Rectus abdominis | Soleus | Trapezius | |
|---|---|---|---|---|---|---|---|---|
| Ease of dissection | Easy | Minimal difficulty | Moderate difficulty | Easy | Easy | Easy | Minimal difficulty | Moderate difficulty |
| Anatomic anomalies | Not important | Not important | No | No | Not important | No | Not important | Sometimes |
| Potential for harvest as compound flap/component tissues that can be included | Yes/skin | Yes/skin, tendon | Yes/skin, bone unusual | Most versatile/skin, rib, scapula bone | Yes/skin, rib | Yes/skin | Not usually | Yes/skin, scapula bone |
| Contour (thin → bulky) | Moderately thin | Moderately thick | Thick | Moderately thick | Moderately thick | Thin | Moderately thick | Thin |
| Potential for thinning | Yes | Yes | Yes | No | No | Difficult due to inscriptions | Yes | No |
| Dynamic transfer | Best | Pedicle transfer | No | Minimal value | Minimal value | Segmental innervation | Pedicle transfer | Yes, for shoulder |
| Donor site morbidity | None | Some, if athletic | Significant, if ambulatory | Minimal | Limited | Can be significant | Some, if athletic | Possible, shoulder drop |
| Surface area | Narrow | Moderate | Small | Largest | Moderate | Small | Moderate | Moderate |
| Vascular pedicle caliber | Moderate | Moderate | Large | Large | Moderate | Large | Small | Moderate |
| Vascular pedicle length | Medium | Medium | Short | Long | Short | Long | Variable | Medium |
| When used as pedicled flap | ||||||||
| Arc of rotation | Moderate | Limited | Limited | Great | Great | Wide | Limited | Great |
| Reliability | Very good | Always | Usually | Always | Very | Usually | Usually adequate | Usually |
| Need for supercharge | No | No | No | No | No | Possible | No | Possible |
| Potential for harvest as distally based | No | Unusual | No | Yes, on secondary pedicles | Yes, on secondary pedicles | Yes, has two dominant pedicles | Only if distal perforator present | No |
| Need for delay procedure | No | No | No | No | Sometimes, if composite flap | Sometimes, if composite flap | No | No |
| Splitting into subportions | Maybe | No | Yes | Yes | Yes | No | Yes | Maybe |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


