29 Congenital hand V
Disorders of overgrowth, undergrowth, and generalized skeletal deformities
Synopsis
• Macrodactyly presents with widely variable clinical pictures, often accompanied with unilateral enlargement, lateral deviations and joint problems. Corrections are difficult and partial. Repeated surgery is often required.
• Brachydactyly is characterized by complex shortening of the digits. The finger shortening ranges from simple undergrowth to total absence of some phalanges. Functional impairment ranges from minimal to severe, when brachydactyly is associated with fusion.
• Constriction band syndrome presents as simple embryonic amputations of digits or soft tissue constricting rings around the fingers or limb. Timely surgical correction is indicated for the simple solitary presentations. Extensive digital losses require special considerations for reconstruction.
• Generalized skeletal abnormalities associated with hand anomalies occur under the categories of a large variety of syndromes, some of which are extremely rare. The management plan depends on the overall clinical picture: decisions should not be made based on the affected hand alone.
Macrodactyly
Macrodactyly is a rare condition in the hand. In Swanson’s classification of congenital deformities of the hand, macrodactyly is labelled as “overgrowth”, in contrast to “undergrowth”, which is also known as hypoplasia.1,2
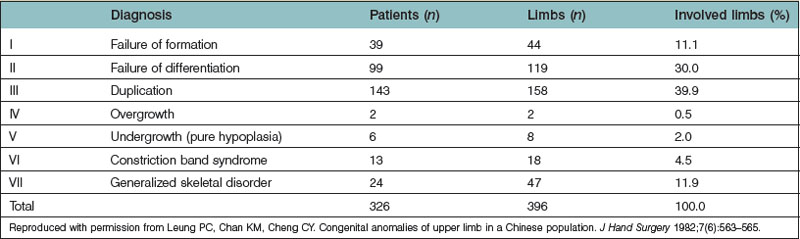
In a survey done in the 1980s, in Hong Kong, on 326 patients presenting with congenital abnormalities of the hand, only two cases were found, comprising only 0.5% of the entire series (Table 29.1).3 The incidence per 10 000 births was estimated to be around 0.2, including all disorders of overgrowth,4 and at the turn of the last century a total of 165 cases of macrodactyly had been reported in the English literature.5 More than one digit was involved in two-thirds of cases and most often, the index and middle fingers were affected simultaneously.
“Overgrowth” or “macrodactyly” is a misleading term. While hypoplasia of the hand has demonstrable undergrowth of the whole hand or component segments of the hand, macrodactyly has a bizarre involvement of segments of the hand unrelated to the anatomical units. In fact, if a finger or a thumb is considered an anatomical unit, macrodactyly does not involve one single unit. Macrodactyly affects either half of the unit, one and a half, or two and a half units. The overgrowth components are the soft tissues. Bone and joint changes, and adjacent tendon and ligament hypertrophies, are secondary effects.6
Surgical dissections have indicated that the major pathology involves hypertrophied digital nerves and their adjacent soft tissues. Histologically, the hypertrophied tissues appear like benign neurofibromas. The correct terminology for “macrodactyly” therefore, might be “digital-nerve orientated benign neurofibroma.”7
If only one digital nerve along one side of a finger is affected, the hypertrophy (macrodactyly) will be confined to that side which will push the un-hypertrophied side away from the mid-line of the finger, causing a severe, whole finger clinodactyly. If the hypertrophy affects the common digital nerve before it divides into digital branches on the adjacent sides of two fingers, both sides of the fingers will be affected, causing divergent clinodactyly.8
The pathology exists since birth and grows rapidly as the child grows, leading to severe deformities, whereby aggressive correction may become necessary (Fig. 29.1A,B). Very rarely, syndactyly occurs together with enlargement (Fig. 29.1C,D), which could be a manifestation of Proteus syndrome (see below).




Surgical correction is complicated and difficult because of the extensive involvement. The policy to be adopted is one of ablation of the abnormal tissues, and reduction or control of the abnormal growth potential of the involved limb. Surgical treatment consists of radical excision of the soft tissues around the digital nerves which might need to be longitudinally split so that only a portion is left intact while the rest is to be ablated together with the soft tissues. Excision of the entire involved nerve has also been performed. When the bones and joints have undergone secondary hyperplasia, shortening with or without excision of one growth plate or fusion of the joint or wedging may have to be done. In the worst case, sacrifice of some digital segment might be necessary. Unless in extreme situations, the involved digit may not need to be sacrificed (Fig. 29.2).8


Macrodactyly and proteus syndrome
There is an unusual form of macrodactyly where there is lipofibromatous hypertrophy of subcutaneous tissues, and the peripheral nerves are not directly involved. The macrodactyly could be localized, but different parts of the body may be more diffusely and asymmetrically involved as in the Proteus syndrome.9 Wiedemann et al. were the first to group the various presentations, naming this Proteus syndrome.10 The genetic cause of Proteus syndrome is still uncertain and debated. It may be a form of genetic mosaicism. It is progressive and is associated with skeletal and vascular changes as well as joint stiffness.11
Brachydactyly
Under Swanson’s classification1 for congenital deformities of the upper limb, Brachydactyly is put under the fifth category of “undergrowth” (hypoplasia). One might have a simple impression that this type of congenital malformation is straightforward under-development. On the contrary, brachydactyly might be the most complicated group of congenital anomalies of the hand. If the undergrowth involves the whole hand evenly, or the entire structure of its major components, e.g., one digit, it would be quite straightforward. However, undergrowth is often affecting only some structures of a digital unit, and moreover, the undergrowth is not infrequently associated with other groups of congenital deformity such as failure to differentiate, failure to form, and duplication. Such complexity may even reach such a stage that classification becomes difficult and priority needs to be subjectively set for proper identification.
In 1951, Bell attempted to classify brachydactyly by distinguishing five main types, which he labeled A, B, C, D, and E (Fig. 29.3).11
B. Apical dystrophy, where there are no nails in the fingers and the thumb is of normal length but broad.
C. “Drinkwater” type, where shortening mainly involves the proximal and middle phalanges of the index and middle fingers.
D. Brachymegalodactyly or stub thumb, where the distal phalanx of the thumb is short and broad.
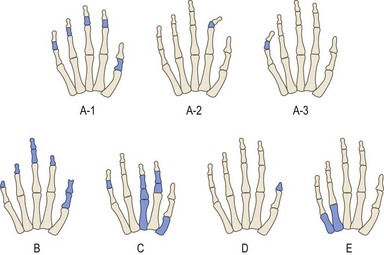
Fig. 29.3 Bell’s classification of brachydactyly.
(Redrawn after Bell J. On Brachydactyly and symphalangism. Cambridge: Cambridge University Press; 1951:1–31.)
Miura12 reviewed 149 cases of brachydactyly of different types in Japan and simplified Bell’s classification by describing them as:
• Brachymesophalangy 5 (that involves the little finger, with 72 cases and was the most common type)
• Brachymesophalangy 2 (that involves the index finger, 19 cases and 7 cases were combined with Brachymesophalangy 5)
• Brachytelephalangy 1 (that involves the distal phalanx of the thumb, 14 cases, and 7 cases were combined with Brachymesophalangy 5)
• Brachymetacarpia (with short metacarpal of different rays, 44 cases, and 36 cases were combined with different types of brachyphalangy).6
When there is brachymetacarpia and brachyphalangy, the condition is usually bilateral and a high proportion of subjects have involvement of their feet as well (Fig. 29.4).
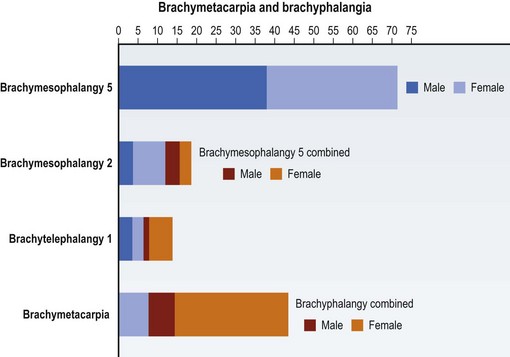
Fig. 29.4 Incidence of different types of brachydactyly.
(Redrawn after Miura T. A clinical study of congenital anomalies of the hand. Hand 1981;13:59–68.)
Brachydactyly could also be related with clinodactyly, i.e., congenital deviation of one finger (Fig. 29.5). The condition frequently affects the middle phalanx of the little finger and is inherited as autosomal dominant. In other situations, the deviation could be the result of a delta shaped middle phalanx. When the index finger is involved, the deviation may be towards the radial side and the condition would be one of Mohr–Wriedt syndrome which is an autosomal dominant congenital anomaly affecting also the feet with clinodactyly or syndactyly (Fig. 29.6).





A delta-phalanx may occur in all digits resulting in the most serious types of brachydactyly and clinodactyly giving functional disabilities (Fig. 29.7).

Other causes of brachydactyly
Shortening of the distal phalanx (usually of the thumb) or shortening of the metacarpals (Brachymetacarpia), unless very severely affected, should not give functional impairments apart from varying degrees of cosmetic concern (Fig. 29.8). Complete absence of the metacarpal, usually the fifth, will cause a grossly deviated little finger and creates a cosmetic and functional problem.

Sometimes the distal phalanx of the little finger is affected. The short distal phalanx then gives a unique palmar-radial curve which has been described as Kirner’s deformity (Fig. 29.9). Brachydactyly is made more complicated when it is associated with syndactyly (Fig. 29.10) and may even be combined with polydactyly (Fig. 29.11).




The combinations of anomalies could be so complicated that undergrowth, failure of formation, failure of differentiation and duplication all co-exist and suggest that a new concept is needed to explain the mechanisms of these deformities. The Japanese Society for Surgery of the Hand, therefore introduced the concept of ‘failure of induction during fetal hand development’ and added a new subgroup to the Swanson classification.1 The description of “brachysyndactyly (or symbrachydactyly)” is included for cases of failure of formation or undergrowth (Fig. 29.12).13,14

Brachymetacarpia
Short metacarpals do not give rise to functional impairment. In some cases, when the shortening occurs in the central digits, the disfigurement becomes striking and parents and child may want correction. If the shortening is mild, elongation may be achieved by a block bone graft in a single operation.15 Elongation for more major deficiency is achieved through the bone transport using a mini-bone distractor.16 Application of this device is awkward because the only site to allow the pins to go into the short metacarpal is the dorsum of the hand. Leaving the distractor in the child’s hand for a few months is not a pleasant experience for any child. The small size of the metacarpal further jeopardizes the lengthening procedures. Family support and persistent counseling will be the key issues to maintain good compliance. Excellent results are not easy to be achieved (Fig. 29.13). The most common problem that could arise from lengthening is loss of motion in the metacarpophalangeal joint.


Symbrachydactyly
In symbrachydactyly, there is the presence of webbed fingers or syndactyly. Occasionally the fingers are very hypoplastic or are absent resulting in just a single digit or a claw like pincer. The procedures for syndactyly release in symbrachydacty are the same as for simple syndactyly. Because the digits are short, the interdigital spaces should be made deeper than usual in order to gain more functional length.17 This is particularly helpful for the first web. The adductor pollicis muscle and the first dorsal interosseous muscle could be released with their insertions and reset to a more proximal site. A dorsal transposition skin flap is frequently required to cover the web and gives good results.18
In severe symbrachydactyly, the middle rays could be rudimentary when the first interdigital space is extremely narrow. In such case, even the most radical web widening procedure might not achieve the purpose of creating a reasonable grip. Consideration should then be given to sacrifice the index ray with ablation (Fig. 29.14).







Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


