27 Congenital hand III
Disorders of formation – thumb hypoplasia
Synopsis






Introduction
For the first 3 months of life, the thumb is adducted and flexed within the palm and serves primarily as a pacifier. By 9 months of age, though, this first ray gains its independence and mobility from the palm, and at a year of age, it has become a crucial portion of the hand.1 In the normal hand, the strength and mobility needed for a wide variety of pinch and grasp functions rapidly develop, and by the time the baby is ambulatory, the thumb is used creatively and independently to manipulate the environment.
As relied upon in the past, a complete evaluation of the osteoarticular column will require plain radiographs. Normal primary ossification centers of the phalanges and metacarpal of the thumb appear in the second to fourth fetal months, but abnormalities of the skeleton of the thumb (e.g., triangular bones) may not be seen radiographically until well into the first or second year of life. Secondary ossification centers within the epiphyses of the thumb normally appear between 13 months to 4 years of age.2 The delayed appearance of both primary and secondary ossification centers in the hypoplastic thumb is highly relevant to the diagnostic process because their appearance is often delayed in proportion to the degree of hypoplasia.
History
In terms of diagnosis and classification, Flatt stressed function potential and designated the digits as “adequate” or “inadequate”3; Bayne relied upon localized positions or deficiencies4; and three generations of German authors referred to the degree of skeletal hypoplasia.5–7 The latter of these three systems recognizes the progressive degree of hypoplasia from a slight size discrepancy, with all normal structures present, to total aplasia of the thumb. In time, this system has been amended by others,8,9 who subdivided type III (severe hypoplasia) into two groups – those with an intact CMC joint (IIIA) and those without (IIIB) – and is very important in terms of management.
Progress in the treatment of thumb hypoplasia mirrored advances in diagnosis and classification. Working independently in Europe, Gosset10 and Hilgenfeldt11 developed the procedure of digital transposition for post-traumatic thumb losses. In the decades following World War II, Bunnell described similar digital transpositions.12 Littler13 refined their techniques and applied them to congenital differences. Following the thalidomide crisis in Europe, Buck-Gramcko14 amassed a large clinical experience and set present day standards for pollicization.
Basic science/disease process
Incidence
The true incidence of thumb hypoplasia is difficult to determine due to the large number of congenital malformations within which a hypoplastic thumb is a component part. All reported reviews are subject to study of the genetic composition of the patient population as well as any discrepancies of nomenclature and sampling. Entin15,16 reported a 16% incidence of thumb hypoplasia in his Canadian patients, while Flatt published an 11.2% incidence of thumb abnormalities and a 3.6% incidence of thumb hypoplasia or aplasia.3 We have seen a 37% incidence within our entire registry, which includes many additional categories.17 The majority of the children treated surgically are those with radial dysplasia – with and without a partial or complete absence of the radius. We have also seen a large incidence in syndromic patients, such as those with the Apert syndrome, who are commonly referred to large children’s hospitals for treatment of their multiple malformations.
Etiology
Because radial or preaxial longitudinal deficiencies occur in many conditions with a wide variety of etiologies, the causes for these malformations span the entire spectrum of genetic, environmental, teratogenic and other factors (Table 27.1). Therefore, consultation with a genetic specialist is strongly recommended, and referral to standard genetic textbooks or the OMIM website18 is a must for any responsible hand surgeon.
Table 27.1 Thumb/radial hypoplasia/aplasia associations
| Frequent in | Occasional in | |
|---|---|---|
| Thumba/radialb hypoplasia/aplasia | ||
| Metacarpal hypoplasia – firstc, alld | ||
| Broad thumb |
The a,b,c,d refers to the hypoplasia/aplasia associations of the listed syndromes. For example, Aase syndrome has both thumb and radial hypoplasia but Nager syndrome has just thumb hypoplasia.
Modified from Jones KL. Smith’s recognizable patterns of human malformations, 5th edn. Philadelphia: WB Saunders; 1997.
Associated conditions
Fanconi anemia and other hematologic abnormalities19
Fanconi (FA) children develop all degrees of a pancytopenia, which can be life-threatening.20,21 Most are small with slow growth. Although many other organ systems may be abnormal, deficiencies of the thumb and, to a lesser extent, the entire radial ray are the most common and are present at birth in over half of these cases. Although in the past FA children were rarely diagnosed early in life, this condition can now be diagnosed at birth with a DEB test.20,22 However, because this test involves an unstable gas, butane, it is not available in all medical centers. Other types of treatable childhood anemias, such as the Blackfan type, may occur in the later childhood years and are easily distinguished by routine hematologic tests including the DEB.21 Treatment of FA children with oxymetholone and prednisone therapy has a 70% response rate, and nonresponders can be treated with bone marrow transplantation.20
Diagnosis and patient presentation
Classification
The varying degrees of differences between hypoplastic thumbs have been classified in a number of ways that have few common characteristics.23 Nevertheless, a well-accepted classification system has emerged that guides treatment. The five designated types of thumb hypoplasia-aplasia are shown in Figure 27.1. These anomalies are commonly associated with radial (preaxial) dysplasia, and the majority of congenital hand surgeons consider most types of thumb with a normal radius as part of this spectrum. It is well recognized that there are concomitant soft tissue anomalies that accompany the skeletal abnormalities. Since the correlation of soft tissue and skeletal deficiencies has been so well defined, this refined system works very well for clinical decision-making.

Hypoplasia of the thumb is associated with many other congenital differences, specifically central and transverse deficiencies. Because the anatomical make-up of the thumb does not always allow for easy categorization under the current system, we have included five additional categories,17 which include the constriction ring syndrome, central deficiencies, radial duplication, the five-fingered hand, and short skeletal rays. In these conditions, the thumb ray usually has characteristic deficiencies that would fall into the German type II and III hypoplasia categories24 and the anatomical abnormalities relevant to clinical decision-making will be presented here.
Clinical presentation (types of hypoplasia)
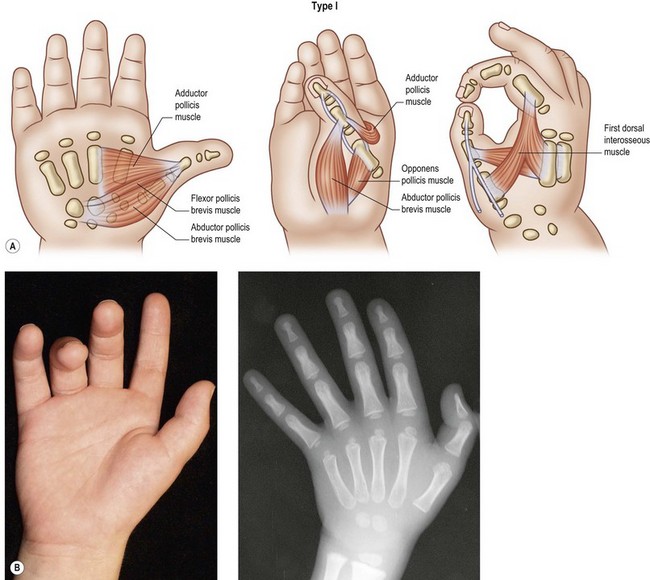
Type I: mild hypoplasia
In this most mild type of hypoplasia, the thumb is slender and slightly shorter than a normally configured first ray (Fig. 27.2). The phalanges and metacarpal can be slightly thinner than usual, but the trapezium and scaphoid are present and the distal radius and styloid process are not affected. The interphalangeal (IP), metacarpophalangeal (MP), and carpometacarpal (CMC) joints are stable and exhibit normal passive and active motion. While there may be a slight hypoplasia and weakness of the abductor pollicis brevis (AbPB), opponens pollicis (OP) and lateral head of the flexor pollicis brevis (FPB) muscles, all intrinsic muscles are present.24 The joints, ligament and capsules, tendons, nerves, and vascular structures are all normal, and there may be minimal narrowing of the first web space.
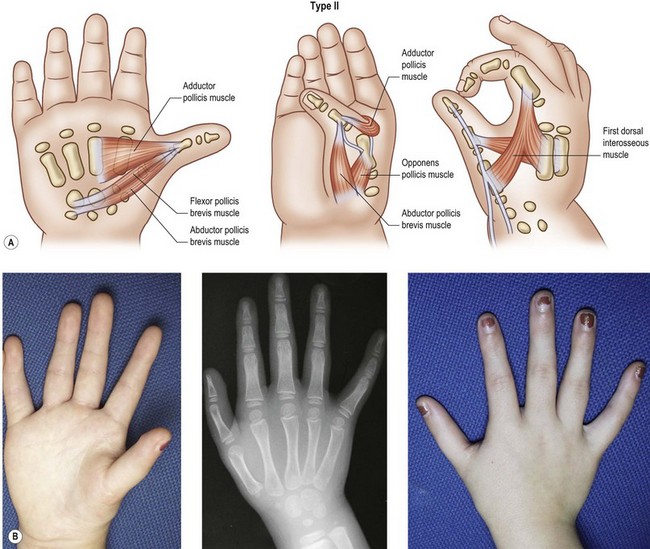
Type II: moderate hypoplasia
The metacarpal and phalanges are all present but small, and the trapezium, trapezoid, scaphoid, and – to a lesser extent – lunate may be hypoplastic. The first web space is short with the thumb adducted, the ulnar collateral ligament at the MP joint lax, and median innervated thenar muscles underdeveloped or occasionally absent (Fig. 27.3).25 Normally, the flexor pollicis brevis (FPB) and opponens pollicis (OP) are innervated by the median nerve, but the FPB varies, reported to be 40% median, 48% ulnar, and 12% both median and ulnar.26 The ulnar innervated intrinsics, particularly the adductor pollicis (AddP), pull the metacarpal into adduction and narrow the first web space, which when explored surgically has tight fibrous bands between muscle groups. Type II thumbs contain two neurovascular bundles, and the recurrent motor branch of the median nerve is consistently found.
Many different muscle and tendon anomalies seen on the radial side of the hand have been identified in conjunction with the type II and IIIA thumbs. In fact, the clinical designation of a given thumb may vary greatly due to this large spectrum of soft tissue abnormalities. Obviously, the absence of interphalangeal (IP) or metacarpophalangeal (MP) flexion or extension creases in a slender thumb is the best clinical indicator of flexor and/or extensor abnormalities. Within this designation, many variations of the long flexor to the thumb (FPL) may be found. Both the tendon and the muscle belly of the FPL may be abnormal,27 may have proximal duplications,28–32 and may have a more radial distal insertion.30 In some patients, one can observe this muscle originating from the index profundus tendon,29 the transverse carpal ligament, or the fascia of the thenar intrinsics and inserting into the flexor sheath28 and/or the extensor mechanism.33 In other cases, this muscle may be absent entirely.9,34–38 Some of these anomalies may represent abnormal radial wrist extensors or short thumb abductors instead of malformed or malpositioned terminal thumb flexors.39 Occasionally, a small abnormal “musculus lumbricalis pollicis” muscle may extend from the thumb origin across the first web space and attach to the flexor system of the index finger.40 We have seen this peculiar (atavistic) muscle extending across the first web space in children with the Freeman–Sheldon syndrome and in complex thumb duplications at the metacarpal level.
In addition, the extrinsic extensors may have abnormal insertions,41,42 extend over the MP joint in a noncentralized position, and reveal abnormal connections with the extrinsic flexor.31,33,40,43 These abnormal insertions of both flexor and extensors, combined with their deviated course, conspire to make both tendons act primarily as radial deviators and not primary flexors or extensors. In addition, the lax ulnar collateral ligament at the MP joint results in an abduction of the phalangeal portion of the thumb. Tupper has called this “pollex abductus” and noted that when these muscles contract, there is no IP flexion or extension, only abduction or radial deviation of the thumb. Many anatomical variations of this structure exist, but the functional result is the same (Fig. 27.4). A recent paper by Graham et al. has summarized the large list of muscle and tendon abnormalities, which often originate in the forearm.31 Although type II thumbs may present with these intra-tendinous connections, the abducted posture and wide degree of muscle and tendon anomalies are primarily seen with type IIIA thumbs (Fig. 27.4). When followed proximally to the wrist and forearm level, many of these tendons have abnormal origins and long muscle bellies that extend well beyond the wrist into the metacarpal region.
Type III: severe hypoplasia
In these cases, the degree of skeletal shortening and narrowing is much more pronounced, particularly at the metacarpal level (Figs 27.5, 27.6). The hand and wrist may be radially deviated due to hypoplastic/aplastic carpal bones. The trapezium is usually very small, and frequently the scaphoid is absent. The distal radius is smaller in size and the styloid process absent, giving the radius a blunted appearance.44 The extreme amount of anatomic variation within this group prompted Manske and colleagues to subdivide this group into type III-A with a full-length metacarpal and an intact CMC joint and type III-B with a tapered first metacarpal and no CMC joint.45 Buck-Gramcko has included an additional variation which we shall call type III-C thumb which possesses only the metacarpal.46 There are no tendons or muscles in this variant, and the skin bridge is much wider than that seen in type IV. In the B and C variants, a fibrous band may connect the hypoplastic metacarpal to a cartilaginous nubbin that represents either a trapezium or metacarpal base. Often, a small abductor pollicis tendon attaches to this remnant.
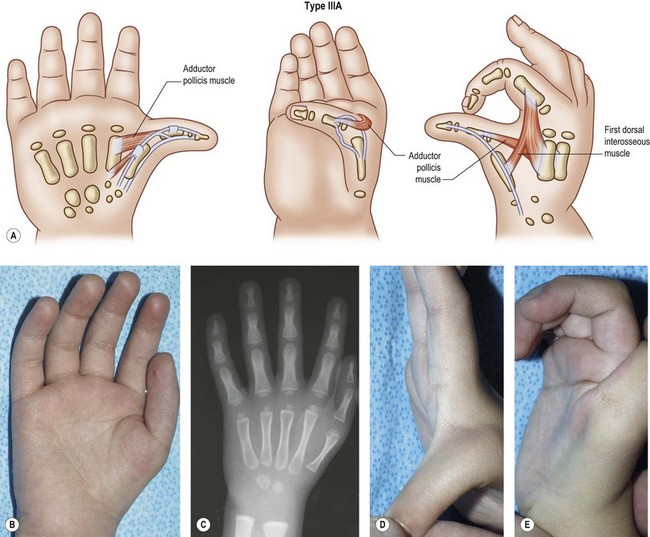
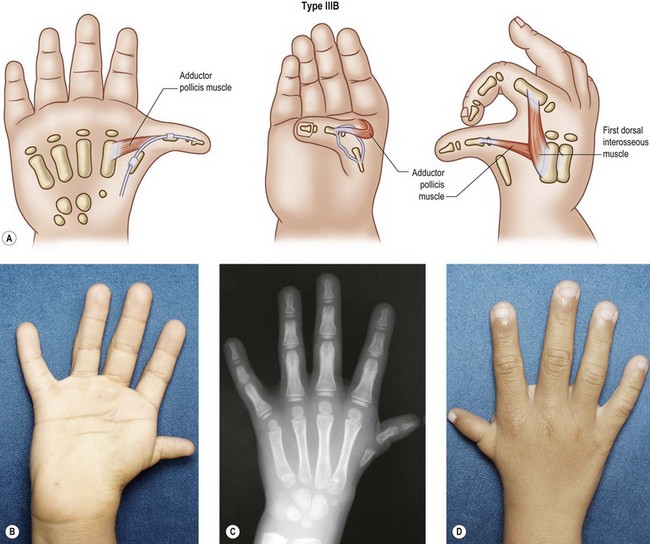
Abnormal anatomy is the rule. The many intrinsic and extrinsic anatomical variations described within the type II group may exist with greater degrees of hypoplasia. Usually, the extrinsic flexor and extensor are present and weak, but in some cases they may be missing.34,38,41 The flexor retinaculum is poorly developed with either attenuation or absence of the major pulleys. In some patients, the motor branch of the median nerve is absent, and there may only be one neurovascular bundle.29 The radial origin of the first dorsal interosseous to the index finger is severely hypoplastic, and the first web space is severely restricted. Pollex abductus anomalies are common and must be recognized if IP flexion and/or extension is to be achieved.
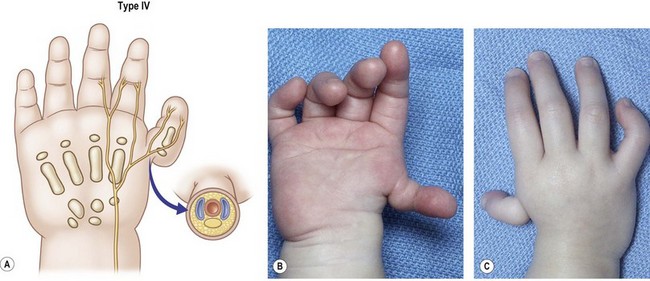
Type IV: floating thumb
These thumbs (pouce flottant, French; pendeldaumen, German) arise distally from the palm and usually lie along the radial midaxial border (Fig. 27.7). They are attached only by a soft tissue pedicle, which has been described by Littler as “Nature’s own neurovascular pedicle,” due to the presence of a digital artery, two vena comitantes, and one or two nerves within the skin bridge.47 There may be anomalous vascular or neural rings, involving neurovascular structures1,5 that could affect the outcome of a pollicization. There is no metacarpal, and two small phalanges tend to be present within the soft tissue envelope, which contains a nail. It is important to note that a diminutive nail represents the presence of a distal phalanx. Intrinsic muscles do not insert onto these bones. A first dorsal interosseous muscle (abductor indicis) may be detected by abduction of the index finger. At the carpal level, the trapezium and less often the scaphoid are missing. The radial styloid may be absent, but the distal end of the radius is normal in most of these children.
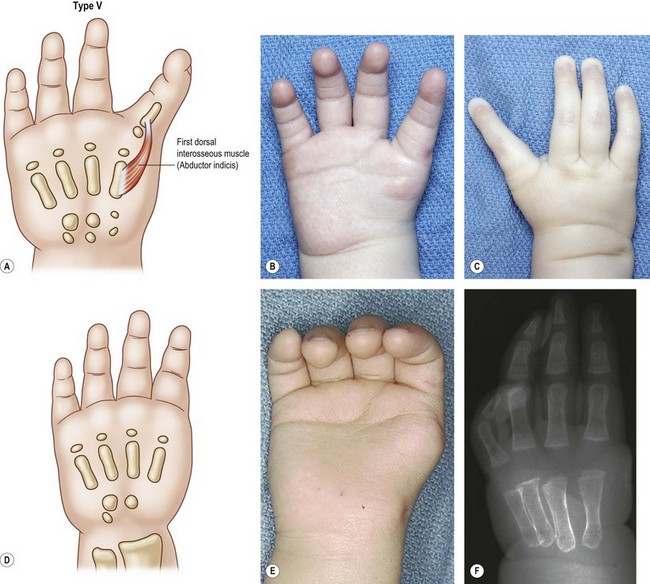
Type V: aplasia
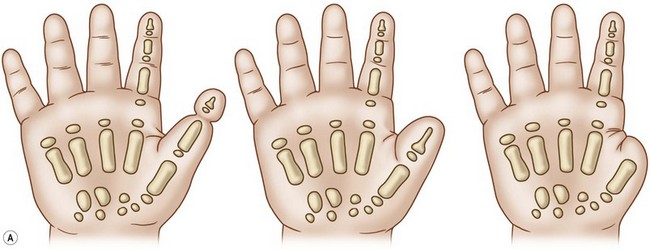
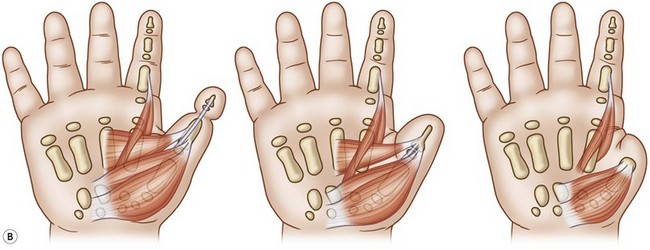
The thumb is completely absent in this category (Fig. 27.8). In half of our patients48 and half those reported by Flatt,49 there is an associated deficiency of the radius. When the radius is normal, the index digit is normal and has strong abduction at the MP joint due to the presence of a strong first dorsal interosseous muscle (e.g., abductor indicis). Many of these children with a normal radius will demonstrate “auto pollicization.” The pulp of the index finger widens and the digit pronates and sits in a more abducted position resulting in a widening of the intermetacarpal space and attenuation of the intermetacarpal ligament. At best, this posture is a poor substitute for normal key pinch. In the case of a deficient radius, the index ray is stiffer, shorter, and often joined by a simple syndactyly to the long digit. There is a direct correlation between the degree of radial hypoplasia and the index finger deficiencies; the index ray is never normal when there are significant associated radial deficiencies. In these hands, the degree of stiffness decreases from the radial to the ulnar digits and the fifth finger is always the best on the hand.
Type VI: central deficiencies: cleft hand and symbrachydactyly thumb
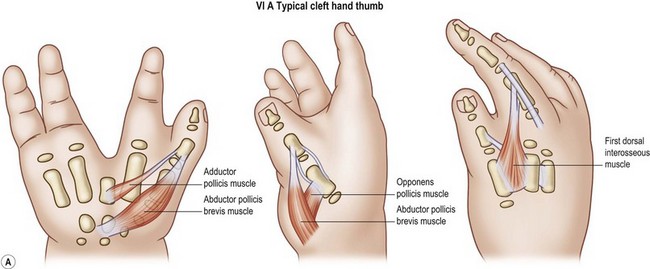
Cleft hand (typical)
Cleft hand is characterized by hypoplasia or aplasia of the central ray(s) of the hand thus forming a “V” or funnel-shaped cleft (Fig. 27.9). All degrees of simple syndactyly of the first web are seen, resulting in moderate to severe deficiencies of the first web space. In addition, all degrees of hypoplasia, extending to aplasia of the central two rays, may exist.9 The ulnar two digits in the ring and fifth positions are commonly webbed with simple syndactylies. The thumb in the cleft hand anomaly is usually slightly small with all components of the osteoarticular skeleton present. A Blauth type II thumb classification would be appropriate for the strict constructionist.24 The wrist and forearm bones are normal, and the median innervated thenar intrinsics are present. The major deficiency of the thumb in this form of hypoplasia is that the ulnar innervated intrinsic muscles are severely hypoplastic or absent. In particular, the ulnar innervated adductor pollicis is usually severely hypoplastic or absent, and the first dorsal interosseous is moderately hypoplastic and contracted. The presence or absence of the third metacarpal is often an excellent indicator of the status of the adductor pollicis muscle. Finally, the extrinsic flexor and extensor musculotendinous units to the thumb tend to be unaffected.

In another variation of typical cleft hand, thumb polydactylies at all levels may be observed. The more distal type I and II polydactylies50 are often associated with the absence of index phalanges that have an intact metacarpal. Super digits and transversely oriented tubular bones at the distal metacarpal level with complete absence of the index (and long) digits are often seen in this variation51 With more proximal type III, IV and V polydactylies, the central (third) ray is often severely hypoplastic or absent.52,53 Triphalangeal rays may also be encountered with the proximal duplications at the metacarpal level.
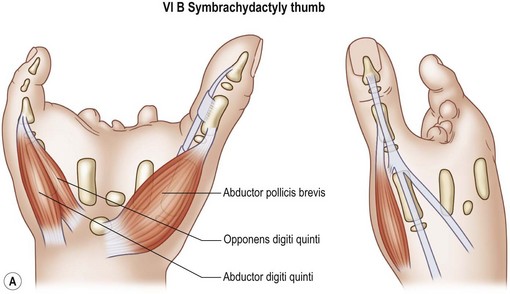
Symbrachydactyly thumb
We refer to these atypical cleft hands as symbrachydactyly (Fig. 27.10). This form of deficiency is always unilateral, with varying degrees of hypoplasia of the central three rays of the hand. Nubbins with minute nail complexes may be present on the distal border of the palm, representing the index, long and ring fingers, but commonly these central three digits are completely absent with varying degrees of hypoplasia of the central three metacarpals.

Type VII: constriction ring syndrome
Amniotic band sequence (constriction ring syndrome, Streeter’s dysplasia) is a condition that can affect one or all limbs and less commonly the face. As defined by Patterson,54 limb involvement can result in any of the following deformities: (1) simple constriction rings, which may be partial or circumferential; (2) constriction rings with distal deformity, with or without concomitant lymphedema; (3) acrosyndactyly (distal fusion, fenestrated syndactyly); or (5) amputation(s) (Fig. 27.11).

Hypoplasia of the thumb is seen in this condition when there is a deficiency in the length of the thumb, which may have a transverse failure of formation at any level. Occasionally, the existing skeletal and soft tissue components of the first ray may be hypoplastic. The hallmark of the amniotic band sequence is that the anatomy proximal to the level of amputation or level of congenital amputation is normal. Either superficial or deep constriction rings around the thumb can be associated with hypoplasia or lymphedema of the distal segment of the digit with hypoplastic nail remnants and slender, truncated phalanges present. Acrosyndactyly is usually seen to involve the central three rays of the hand but can also involve the thumb and fifth finger. Amputation of the thumb in this condition is the major cause of partial aplasia of the thumb and can occur at any position along its length. The most practical way to analyze the amputation is to place it at one of three levels: (1) distal to IP joint; (2) proximal phalanx, and (3) metacarpal (Fig. 27.11). Motion of the IP joint is usually severely affected – even with amputations or deep constriction rings distal to it.
Type VIII: five-fingered hand
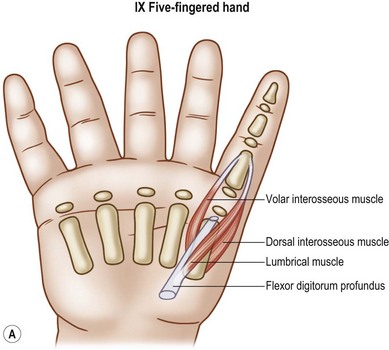
In this type of hypoplasia, the thumb is smaller in width and longer in length and has the characteristics of a finger. As the radial border digit, it lies in the same plane as the ulnar four digits and is nonopposable. It is usually the same length as the adjacent index finger. The digit is slender and may be joined to the index finger in an incomplete simple syndactyly. A severe deficiency or nonexistent first web is often present, and some type of transverse metacarpal ligament is also present. The skeletal anatomy is similar to that of the index ray: a metacarpal with a distal growth center and three phalanges with proximal growth centers. The scaphoid is usually absent or hypoplastic. The thenar musculature (AbPB, FPB, OP muscles) are also absent as is the adductor pollicis (AddP). Instead, the usual digital intrinsics are present – namely, a lumbrical, palmar, and dorsal interosseous (Fig. 27.12). The extrinsic flexors and extensors mimic those of the normal fingers. Because the radial digit lies in the same plane as the other fingers in the hand, manipulation of objects is usually performed by utilizing lateral scissoring between the first two digits – or between the second and third if a first web syndactyly is present. Left untreated, those patients without a first web syndactyly tend to attenuate the transverse metacarpal ligament and “autopollicize” into an abducted and slightly pronated posture.

Type IX: radial polydactyly
Musculotendinous abnormalities are common with the extrinsic extensor almost universally shared. Indeed, nearly half of the patients presented in papers on pollex abductus involve duplicate thumbs.40,43 Deviation of the partners toward each other indicates abnormal insertions of the extrinsic tendons into the distal phalanges, and connections between the extrinsic flexors and extensors are not unusual. These tendinous interconnections will limit function and cause digital angulations. The first web is usually unaffected in polydactylies involving the distal phalanx, but as the level of arborization lies more proximally, the first web space becomes increasingly deficient and tight.
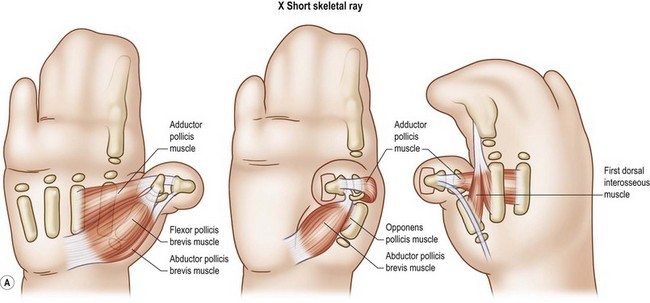
Type X: syndromic short skeletal thumb ray
Deficiencies of the osteoarticular column of the thumb may result in a short, hypoplastic thumb (Fig. 27.13). Bony abnormalities can occur as isolated bone (brachymetacarpia, brachyphalangia), all bones in combination, or as part of a generalized syndrome, such as the acrocephalosyndactyly (e.g., Apert, Pfeiffer, Carpenter, etc.) syndromes or the Rubinstein–Tabyi syndrome. Joint function is usually impaired on either side of the abnormal bone(s). In patients with anomalies of a single bone, brachymetacarpia or brachyphalangia, the remaining components of the thumb tend to be unaffected, and in patients with generalized syndromes, other abnormalities of the thumb components are common. In the acrocephalosyndactyly (ACS) syndromes, delta phalanges are common. They usually involve the proximal phalanx with a longitudinal epiphyseal bracket on the radial side. This abnormal growth plate checks growth on the radial side and results in a radial clinodactyly of the thumb, which becomes more severe over time. The metacarpal is usually short and the distal phalanx is short and broad. Incidentally, many feel that the abnormal proximal phalanx and broad distal phalanx are variations of a polydactyly. Musculotendinous anomalies are associated with poor joint function but are not as common as those with type IIIA thumbs. Deficiencies of the first web are most common, occurring along a spectrum of mild adduction contracture to complex syndactyly involving the first two rays.

Patient selection
General considerations
The child with thumb hypoplasia may present many unique problems with both pinch (precision, pulp, key) and grasp (precision, span, power), despite his/her ability to adapt remarkably to the functional deficiency.23 The ideal prerequisites for reconstruction of a functional thumb include55:
1. A mobile, stable CMC joint with an intact metacarpal
2. A scar-free first web space of adequate width and depth lined with full thickness skin
3. Mobility in at least two of its three joints (CMC, MP, IP)
4. MP joint stability, particularly of the ulnar collateral ligament
5. Adequate motors for strong MP or IP flexion and extension
6. Capacity to be placed in a palmar abducted (i.e., opposition) position for pinch and grasp maneuvers.
All six of these components should be considered in any detailed analysis of the thumb.
Timing
As researchers and clinicians struggle with the possibilities of fetal surgery, many surgeons wonder if they should wait rather than performing reconstructive procedures of the congenitally different hand as soon as possible (Fig. 27.14). Early reconstruction of the hypoplastic or absent thumb is certainly attractive in an effort to allow the infant to adapt more rapidly with optimal cortical representation. This ideal needs to be tempered with the knowledge that a congenital hand difference is, in itself, not a life-threatening condition (but may be associated with one), and the surgeon can use time to allow the affected part to grow, to observe development, and to assess the functional needs. The construction of the thumb with a stable osteoarticular column of adequate length, mobile joints, growth potential, scar-free first web, and gliding muscle tendon units is not easily accomplished in very small hands – despite our refined microvascular instruments and skills.

However, the arguments that are forwarded by the proponents of the early surgery persist. Among the most powerful points include anatomic, cognitive, and psychological factors. Anatomically, the release of tethered musculotendinous units and joint contractures will allow unrestricted growth, and physiological adaptation of the reconstructed thumb will occur secondary to growth and functional use.55 On a cognitive level, early surgery will allow the development of the child with a reconstructed thumb to occur prior to thumb corticalization, which takes place at around 18 months of age. Psychologically, correction will alleviate anxiety in the parents and, therefore, in the child.
In the absence of other organ system complications, we try to reconstruct these problems when the child is between 10 and 18 months of age. Pollicization at 1 year is often preceded by centralization of the hand and wrist between 5 and 8 months of age in those with radial deficiency. The timing for correction of type IIIB deformities may be problematic. Though pollicization is the procedure of choice, some parents and families simply will not allow it. We agree with other surgeons that the alternatives involve difficult reconstructions, often including one or more stages, and are wisely deferred until the child is aged 4–5 years, a time when the hand is larger and the patient may be more cooperative with the postoperative therapy regimen.5,23,31
Treatment
Treatment considerations for thumb hypoplasia (types I–V)
Type I: mild hypoplasia
These children are not usually functionally impaired (Fig. 27.2). In fact, many type I thumb hypoplasia patients, along with their parents, do not recognize anything abnormal about these hands. These thumbs are commonly found in patients who have a more severe radial dysplasia in the opposite upper limb. However, in this stronger limb, they have very little or no difficulty with key pinch, pulp to pulp pinch, opposition and grasping activities. Since functional problems are rare, surgical correction is not often needed. Occasionally, a child with a type I hypoplastic thumb will require a release of a mildly contracted web (see Type II management). All web releases involve more than simple skin incisions. Careful56 attention must be directed to tight fascial bands within the web space, anomalous tendon and muscle anatomy and joint ankylosis. Of all the methods available, the 4-flap Z-plasty provides the best contour and appearance (Fig. 27.15). Dorsal transposition flaps from the index finger34 and rotation flaps56,57 are effective but require skin grafting on the visible dorsal surface of the hand. Of course, any method must be carefully individualized to the patient.
Type II: moderate hypoplasia
 Video1
Video1Five specific problems in the type II thumbs must be addressed individually: (1) narrowed first web space; (2) instability of the MP joint; (3) poor palmar abduction (opposition) for pinching and grasping; (4) lack of IP joint flexion, and (5) abduction posturing of the thumb (“pollex abductus”) (Figs 27.3, 27.4). Usually, all that is needed to correct these thumbs is a release of the first web space and stabilization of the MP joint, with or without a transfer for palmar abduction or opposition. When the surgeon encounters a pollex abductus deformity, she/he should next look for abnormalities of the flexor pollicis longus (FPL) muscle. A more detailed description of treatment options is presented later in this chapter.
Type IIIA: severe hypoplasia
Most hand surgeons agree that this variation should be reconstructed surgically (Fig. 27.5). The five individual problems are the same as listed in type II, and the options and preferred solutions are listed below. Most authors opt to complete all necessary procedures including widening of the first web space, stabilization of the MP joint, and some type of opposition transfer at one time. The major variable becomes the status of the flexor mechanism, which may require a staged approach. After 35 years of experience, our preference has been to replace the very anomalous flexor mechanism with a tendon transfer in the presence of at least one good pulley at the level of the metacarpal head. The treatment of the more deficient type IIIB and IIIC varieties constitutes one of the more interesting ongoing controversies in hand surgery.
Type IIIB, type IIIC: severe hypoplasia
For most hand surgeons in Europe, North America and South America, pollicization is the treatment of choice because a well-performed pollicization provides a much better and more predictable outcome than any alternative types of staged reconstruction (Fig. 27.6).
However, cultural and parental beliefs may demand one of two alternatives – staged reconstructions with58–61 and without62 a microvascular joint transfer, which have both become popular in the Asian countries. Osteoplastic thumb reconstruction has a long history.6,63–65 The osteoarticular column is connected with an intercalated bone graft between the index and hypoplastic thumb metacarpal (Fig. 27.16). Multiple stages are then needed to first stabilize MP and IP joints and construct pulleys. At that point, tendon transfers are performed for opposition as well as IP flexion and extension. The major disadvantages of this procedure include the lack of CMC mobility, lack of growth, poor motion and the multiple stages required. Insensate abdominal pedicle flaps have been used to provide tissue for an adequate first web space.

Another alternative is to transfer either the second62,66–69 or third70 or first metatarsophalangeal joint in a hyperextended position to create a new CMC joint and proximal metacarpal. This composite joint must be harvested with a large dorsalis pedis pedicle, which provides venous drainage and adds bulk to the deficient thenar region. Tendon transfers are then performed to provide motion at either the MP or IP joints.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


