The musculoaponeurotic layer of the abdominal wall should be corrected during abdominoplasty according to the specific deformity that the patient presents with. In this article, the anatomic basis of deformities and defects of the abdominal wall is described. Different degrees of deformities secondary to pregnancy are described as well as congenital muscle malposition. These conditions should be treated in specific ways so that the most efficient correction can be achieved and no recurrence will occur. In cases of associated incisional hernias, the ‘‘components separation’’ technique can be considered for abdominal wall reconstruction and 2 alternative techniques of dissection of myoaponeurotic components are described for the correction of specific defects.
The abdominal wall may be affected by pregnancies, weight variation, and previous abdominal surgical procedures. Some patients may present, in addition, a weakening of the musculoaponeurotic layer attributable to aging or to a congenital condition. These factors alter the cosmetic aspect of the abdominal wall and its function. Plastic surgery of the abdomen should restore function providing a balance between the anterior and posterior muscles of the abdominal wall and improve the cosmetic aspect. As patients’ deformities differ, abdominoplasty has become a customized operation since its initial description. This article focuses on recognition of the different deformities of the musculoaponeurotic layer of the abdominal wall and their treatment.
The role of the extracellular matrix on the deformity of the abdominal wall
Deformities of the musculoaponeurotic layer are a result of acquired, congenital, and genetic conditions. Each one of these plays an important role in the etiology of the deformity. Therefore, it is important to recognize them and offer the patient a specific treatment. However, it is not possible to surgically correct every abdominal deformity. Some patients present such a weak aponeurosis that surgical correction is impossible. The ratio of collagen type I and III in the composition of aponeurosis is a genetic condition and there is also a change in this relation with age. This change is attributable to the increase in the number of type III collagen fibers as compared with the number of type I fibers. It has been shown that aponeuroses with a high concentration of type III fibers are weaker than those with a higher rate of type I fibers.
Another factor that may play a role in the correction of the musculoaponeurotic layer is the collagen deposition in muscles. Collagen within the muscles (types I, III, IV, and V) is located in the epimysium, perimysium, and endomysium. With age there is an increase in the total number of fibers and the muscles become less flexible and pliable. This may increase resistance to mobilization of the muscles during correction of abdominal deformities.
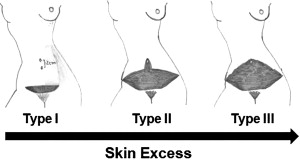
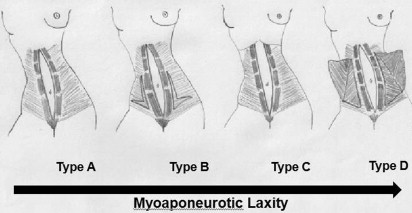
Also, it is important to stress that there is a relationship between the musculoaponeurotic deformity and the skin excess of the abdomen. Patients with large skin excess present more complex musculoaponeurotic deformities. This occurs because the quality of the extracellular matrix of skin, aponeurosis, and muscles has similarities in the same individual. A visible example of that is when 2 abdominal deformity classifications are compared in the same group of patients. The first abdominal deformity classification evaluates skin excess and is based on 3 different types of skin deformities. Type I patients present mild excess skin with a high-positioned umbilicus. Type II patients have mild excess skin and a well-positioned umbilicus as well as those with moderate excess skin. Type III patients present severe excessive skin ( Fig. 1 ). Another classification, based on musculoaponeurotic deformities, separates patients into 4 different types. Type A patients are those who present rectus diastasis secondary to pregnancy, and are followed by types B, C, and D with gradually more complex musculoaponeurotic deformities ( Fig. 2 ). Therefore, type A and I patients are those with more subtle deformities, whereas type D and III present a more severe deformity. Table 1 shows the same patients classified using both classifications. It is possible to verify that more severe skin deformities are related to more complex musculoaponeurotic deformities.
| Skin Deformity | n (%) | Myoaponeurotic Deformity | n (%) |
|---|---|---|---|
| Type I | 3 (3.6) | Type A | 3 (3.6) |
| Type II | 24 (28.9) | Type A | 15 (18.1) |
| Type B | 6 (7.2) | ||
| Type C | 3 (3.6) | ||
| Type III | 56 (67.5) | Type A | 46 (55.5) |
| Type B | 4 (4.8) | ||
| Type C | 4 (4.8) | ||
| Type D | 2 (2.4) | ||
| Total | 83 (100) | 83 (100) |
Brauman has shown that the correction of diastasis does not reflect a good cosmetic result in all cases, even if there is no recurrence of the diastasis with time. The possible reason for this is that the quality of collagen differs in each individual.
Surgical treatment of the myoaponeurotic layer of the abdominal wall
A specific treatment is described for each type of deformity of the musculoaponeurotic layer.
Type A patients present a rectus diastasis typically secondary to pregnancy on which there is a fusiform diastasis (see Fig. 2 ). Both recti muscles are inserted on the costal margins close to the midline. In these cases the plication of the anterior rectus sheath is used to correct diastasis.
Type B patients are those who present a bulging of the musculoaponeurotic layer after the correction of diastasis. These patients may present vertical elongation of the abdominal wall. Patients who need some improvement in the waistline may also reap the benefits of this technique. To correct these deformities an “L”-shaped plication of the external oblique aponeurosis should be done in addition to the plication of the anterior rectus sheath (see Fig. 2 ).
Type C patients present a congenital rectus diastasis. In these cases the recti muscles are inserted laterally in the costal margins. The recti muscles should be advanced in this case (see Fig. 2 ).
Type D patients present a poorly defined waistline and a strong aponeurosis of the external oblique muscle. To improve the waistline, advancement of the external oblique muscles should be performed in addition to plication of the anterior rectus sheath (see Fig 2 ).
Therefore, these techniques are used for each patient, depending on the specific deformity. This classification has been used in other studies on the musculoaponeurotic treatment of the abdominal wall.
The techniques used for correction of the specific abdominal deformities and defects are described in the following sections. Also, the studies that support the aponeurotic plications and muscle advancements are discussed.
Plication of the Rectus Sheath
The most complex deformity after pregnancy is the patient who present a rectus diastasis associated with little excess skin and a thin adipose tissue layer. Although this deformity is rare, this type of patient has always been a challenge for plastic surgeons, as skin removal is limited and a large incision should be performed to allow access to the area of diastasis. In 1993 we described a different approach to treat these patients. A laparoscopic technique was used to correct rectus diastasis. This technique was used to avoid the undermining of the abdominal flap where there are several perforator arteries, mostly around the umbilicus. The plication was performed in the posterior rectus sheath after the peritoneal incision. This technique was tested in cadavers and swine, and after that it was used in human beings. Its indications are few and it is rarely used.
The plication of the anterior rectus sheath is the most frequent procedure performed by plastic surgeons to correct deformities of the musculoaponeurotic layer; however, its efficacy was not verified until 1981. In that year, Birdsell and colleagues checked the position of the recti muscles after the correction of diastasis using metal clips on the medial edges of the recti muscles. Their position was checked using radiographs. However, there was some criticism of this method of evaluation as the metal clips could be involved by fibrosis and their final position on the radiograph could mislead their real location. Therefore, it is possible that the diastasis could have recurred even if the clips were close together in the midline within the fibrotic area. With the purpose of verifying whether the plication of the recti muscles using nonabsorbable suture (2-0 nylon) could be an effective procedure to correct rectus diastasis, a study was conducted by the senior author (F.X.N.) using CT scan to verify the 6-month postoperative position of the muscles at the supraumbilical and at the infraumbilical areas. The results showed that there was total correction of diastasis using this technique. Another study was done by the same group using absorbable sutures (polidiaxonone [PDS]; Ethicon, New Brunswick, NJ, USA) and similar results were obtained after 6 months, showing correction of diastasis in all patients.
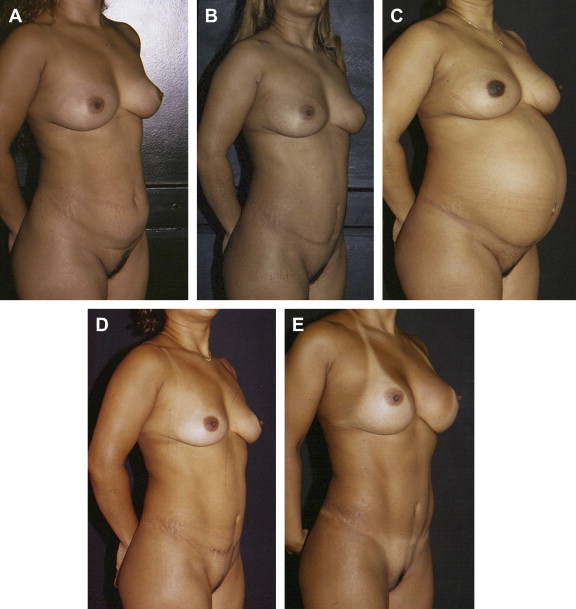
It has been shown that correction of diastasis by plication of the anterior rectus sheath can even resist the pressure of intra-abdominal expansion during pregnancy. It is not possible to ensure that every patient who gets pregnant will not have recurrence of the diastasis as the one described in the article. However, in this particular patient, there was enough fibrosis in the area of the plication 2 years after the procedure. The fibrosis kept the recti muscles together in the midline and there was normal fetal growth as the expansion of the surrounding tissues occurred. Because there are muscles and aponeuroses in the surrounding tissues, there is a better chance of retraction of the tissues after delivery. Four months after delivery the patient was oriented to exercise and, as she did not have diastasis, there was good improvement of the abdominal contour without the need of any other abdominal procedure ( Fig 3 ).
Related posts:
 Anatomic Considerations in Abdominoplasty
Anatomic Considerations in Abdominoplasty
 Editorial Comment on “Traditional Abdominoplasty”
Editorial Comment on “Lipoabdominoplasty: The Saldanha Technique”
Editorial Comment on “ SAFECircumferential Liposuction with Abdominoplasty”
Editorial Comment on “Concepts on Correction of the Musculoaponeurotic Layer in Abdominoplasty”
Revision Abdominoplasty and Proper Umbilical Positioning
Editorial Comment on “Traditional Abdominoplasty”
Editorial Comment on “Lipoabdominoplasty: The Saldanha Technique”
Editorial Comment on “ SAFECircumferential Liposuction with Abdominoplasty”
Editorial Comment on “Concepts on Correction of the Musculoaponeurotic Layer in Abdominoplasty”
Revision Abdominoplasty and Proper Umbilical Positioning
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


