3
Common Pathological Conditions of the Pediatric Craniovertebral Junction and Cervical Spine
 Down Syndrome
Down Syndrome
Etiology
Trisomy 13 is the recognized cause of Down syndrome.
Natural History
Atlanto-occipital motion There are no data examining the natural history of atlanto-occipital motion in Down syndrome patients. Fusion is recommended for atlanto-occipital motion greater than 10 mm.1
Atlantoaxial motion The amount of C1–C2 motion remains constant over time in patients with Down syndrome once they reach ~6 years of age.2–4 There are no data examining the natural history of atlantoaxial motion before that age. Fusion is recommended for excessive C1–C2 motion, as evidenced by an atlantodental interval greater than 6 to 8 mm or a neural canal width less than 12 mm.1
Subaxial motion Idiopathic subaxial instability in Down syndrome is rare.5 There are no data examining its natural history.
Common Anatomical Idiosyncrasies
The atlanto-occipital joint in Down syndrome is characterized by a “rocker-bottom” configuration, with flat, wide occipital condyles and flat C1 articular surfaces (Fig. 3–1). This anatomy contributes greatly to atlanto-occipital instability. The atlas has many anatomical variants in Down syndrome, although an absent or split posterior arch or a bifid arch (leading to two hemi-rings) are the two most common (Fig. 3–2). The axis may have odontoid abnormalities such as os odontoideum or a hypoplastic dens (Fig. 3–3).
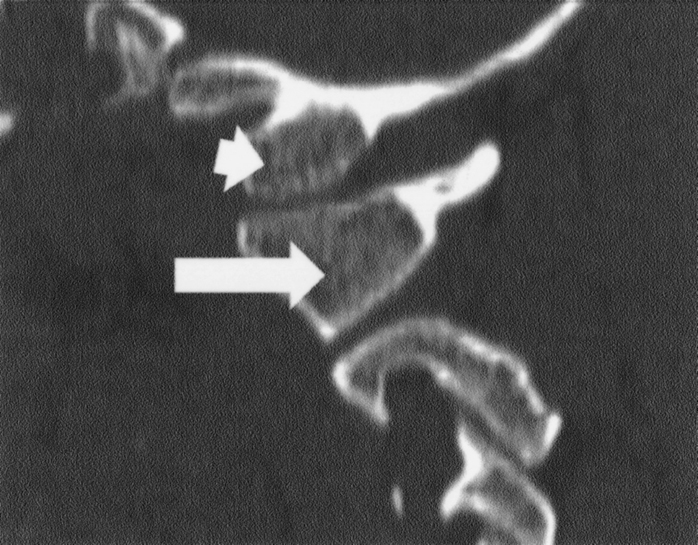
Figure 3–1 Parasagittal two-dimensional computed tomographic reconstruction of the occipital condyle in a typical patient with Down syndrome. It is thought that the anatomical configuration of this type of joint leads to congenital occiput–C1 instability. (arrowhead) Occipital condyle; (arrow) C1 lateral mass.
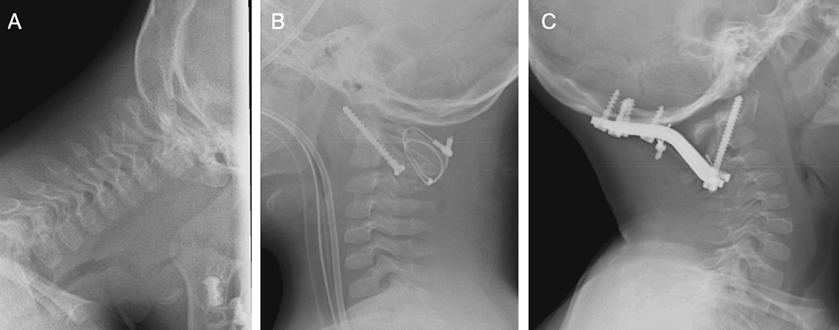
Figure 3–2 (A) A 3½-year-old boy with Down syndrome and atlantoaxial instability. Note congenital absence of posterior C1 ring. (B) Postoperative lateral cervical spine film after first fusion attempt showing C1–C2 transarticular screws and posterior bone-and-cable fusion. (C) Postoperative lateral cervical spine x-ray showing second attempt at fusion with occipital–C2 construct, using C1–C2 transarticular screws and Avery-Brockmeyer-Thiokal plate (Medtronic Sofamor Danek, Minneapolis, MN).

Figure 3–3 An 18-month-old girl with Down syndrome and severe atlantoaxial instability secondary to congenital atlantoaxial instability. (A) Preoperative lateral plain film, showing severe atlantoaxial instability. (B) Preoperative midsagittal T2-weighted magnetic resonance imaging, showing narrowing at the craniovertebral junction. (C) Postoperative lateral plain x-ray, showing C1–C2 transarticular screws and posterior bone-and-cable “girth-hitch” arthrodesis.
Surgical Considerations
Posterior C1–C2 transarticular screw fixation is an excellent method to provide internal stability for Down syndrome patients at almost any age. However, care must be taken in patients with posterior C1 arch abnormalities because there may not be enough bone available to provide an environment for adequate fusion. For patients with atlanto-occipital instability, an occiput to C2 fusion with internal fixation, such as the Avery-Brockmeyer-Thiokol (ABT) plate (Medtronic Sofamor Danek, Minneapolis, MN ), is a very good construct.
 Klippel-Feil Syndrome and Klippel-Feil Variant
Klippel-Feil Syndrome and Klippel-Feil Variant
Etiology
The etiology of Klippel-Feil syndrome and Klippel-Feil variant is unknown. Multiple theories have been proposed, but a vascular etiology seems most likely.6,7
Natural History
Instability caused by intrinsic abnormalities of the craniocervical joints may progress over time. One study found cervicothoracic fusions to be a risk factor for progressive instability.8 Adjacent level instability may occur after fusion of any craniocervical segment (Fig. 3–4).

Figure 3–4 A 10-year-old girl with Klippel-Feil syndrome, with a history of previous anterior cervical diskectomy and fusion from C3 to C7. (A) Plain lateral cervical spine film in flexion, showing significant incursion of the occiput on C2. (B) Plain lateral cervical spine film in extension, showing reduction of deformity from the previous figure. (C,D) Parasagittal two-dimensional computed tomographic reconstructions through the occipital condyle of the (C) right and (D) left C1–C2 regions, respectively. Note the extremely flat shape of the occipital condyle/C1 region. (E) Postoperative plain lateral cervical spine film, showing occiput–upper cervical spine fusion using Ohio Medical Instruments (OMI) loop (Ohio Medical Instruments Company, Inc., Cincinnati, OH) and C1 lateral mass screws bilaterally.
Common Anatomical Idiosyncrasies
Klippel-Feil syndrome and its variants are commonly associated with occipitalization of the atlas, Chiari I malformation, and a wide variety of complex, sometimes bizarre, cervical bony abnormalities (Figs. 3–5, 3–6, and 3–7). Bone quality is typically normal.
Surgical Considerations
As a group, Klippel-Feil syndrome patients present with a wide variety of craniocervical pathologies, leading to use of the entire spectrum of craniocervical surgical techniques. Great care must be taken in the preoperative phase to understand the patient’s anatomy so that surgical planning takes into account all possible ways of achieving stability. The surgeon will be significantly challenged in a high percentage of cases.
Related posts:
 Advanced Occipitocervical Surgery in Children
Advanced Occipitocervical Surgery in Children
 Advanced Atlantoaxial Surgery in Children
Advanced Atlantoaxial Surgery in Children
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


