Acne scarring is physically and psychologically distressing to patients, and treatment of acne scarring remains a clinical challenge. Most patients have multiple types of acne scarring, so a multimodal approach to treatment is often recommended. This paper explores the role of combining non-ablative fractional lasers (NAFL) and microneedling with radiofrequency (MNRF) for the treatment of acne scarring. Combined NAFL+MNRF demonstrate promising results with significant improvements demonstrated in the literature. Further research is warranted to determine the appropriate combination regimen to integrate into clinical practice to optimize patient outcomes.
Key points
- •
Most patients suffer from a combination of acne scar types, so a multifaceted approach to treatment is generally recommended to optimize outcomes.
- •
Ablative lasers are generally regarded as the gold standard for facial resurfacing; however, the downtime and side effect profile limit their use in clinical practice.
- •
Both non-ablative fractional lasers (NAFL) and microneedling with radiofrequency (MNRF) show significant and similar improvements in acne scaring.
- •
Combining NAFL and MNRF leverages distinct mechanisms of action, aiming to improve the efficacy of treatment for acne scarring.
- •
Combined NAFL+MNRF treatment shows significant improvement in acne scarring, though further studies are needed to clarify the difference in efficacy between combined treatment and monotherapy.
Introduction: nature of the problem
Acne vulgaris is one of the most common inflammatory skin disorders, affecting an estimated 95% to 100% of adolescent boys and 83% to 85% of adolescent girls, often continuing into adulthood [ , ]. Acne scarring—a frequent and often permanent consequence—impacts up to 95% of individuals with acne vulgaris [ ]. Scarring varies from mild to severe, with approximately 30% of patients presenting with more severe forms.
Acne scarring can cause a substantial physical and psychological burden. Numerous studies have highlighted the emotional toll of acne scars, with patients reporting higher rates of anxiety, depression, and diminished self-esteem [ , ]. Profound psychosocial consequences can influence self-confidence, social interactions, relationships, academic performance, and professional life ( Fig. 1 ) [ ]. Given the high incidence of acne scarring, as well as the detrimental impact on patient quality of life, effective treatment options are critical.

Acne vulgaris induces chronic cutaneous inflammation, which disrupts the balance between matrix degradation and collagen synthesis, leading to the formation of scars [ ].
Acne scars can be broadly categorized into hypertrophic or atrophic types.
- •
Hypertrophic: result from excessive collagen production and can develop into keloidal or raised scars.
- •
Atrophic: result from insufficient collagen deposition and can develop into 3 subtypes of scars.
Atrophic scars are more common, accounting for 80% to 90% of acne-related scarring [ , ]. They are further subclassified into ice pick (V-shaped), boxcar (U-shaped), and rolling (M-shaped) scars, each with distinct morphologies and treatment challenges ( Fig. 2 ) [ ]. In most patients, a combination of these scar types is present, requiring a multifaceted approach to treatment.
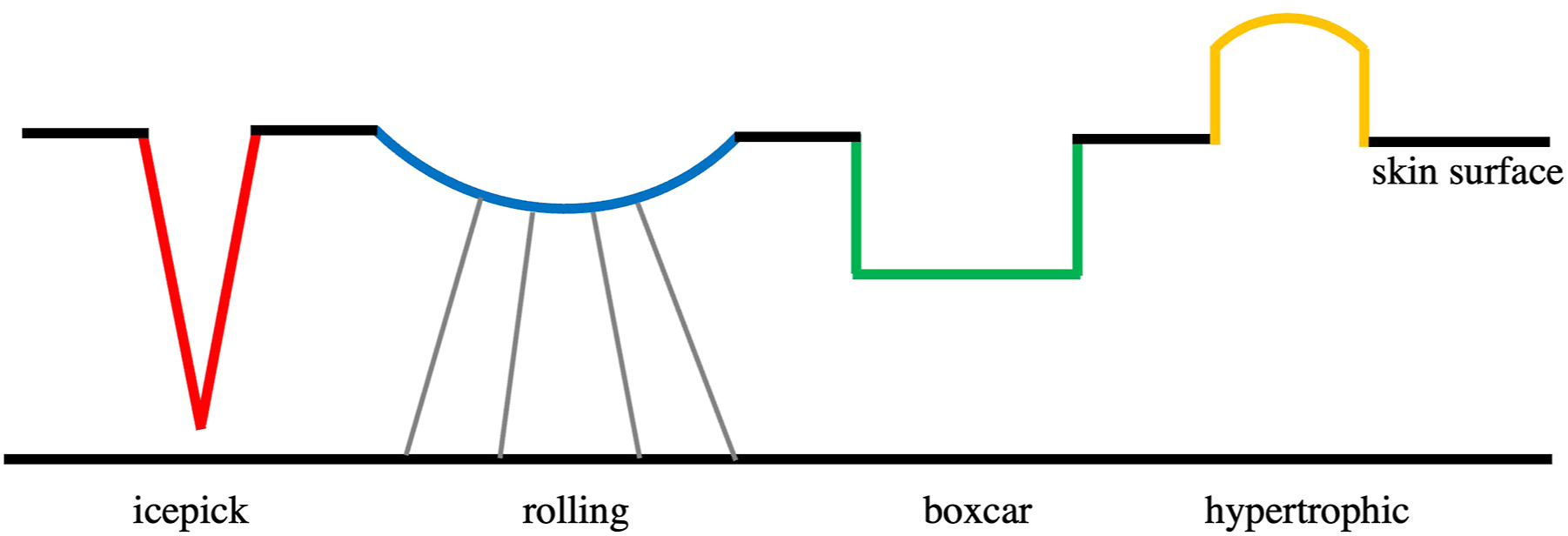
Atrophic subtypes.
- a.
Ice pick: most common type (60%–70%)
- i.
Narrow and deep
- ii.
Least responsive to treatment
- i.
- b.
Boxcar: second most common type (20%–30%)
- i.
Broad and shallow (can be deep)
- ii.
Most responsive to treatment
- i.
- c.
Rolling type: least common type (15%–25%)
- i.
Wave-like or undulating appearance due to fibrous septa tethering the overlying skin to the fascia
- ii.
Moderately responsive to treatment
- i.
A wide range of therapeutic options is available for addressing acne scars, including: non-surgical techniques such as dermal fillers, chemical peels, dermabrasion, microneedling, and platelet-rich plasma injections; surgical procedures such as subcision, punch excision, punch grafting, punch elevation, and elliptical excision; and energy-based devices, such as ablative fractional laser (AFL), non-ablative fractional laser (NAFL), and microneedling with radiofrequency (MNRF) [ , ]. Among these, energy-based devices have become central to treatment of acne scarring and are increasingly recognized as first-line treatments.
Ablative non-fractional lasers and AFL, such as carbon dioxide and erbium lasers, are considered the gold standard for resurfacing. Ablative lasers deliver a wavelength of light that vaporizes the epidermis and dermis, with the dermal penetration depending on the depth and energy selected by the clinician [ ]. AFL utilizes fractional thermolysis to create microthermal treatment zones with this wavelength of light, with the interspersed untreated epidermis and dermis helping to reduce downtime and speed re-epithelialization [ ]. Ablative non-fractional lasers, AFL, and, more recently, combination AFL + MNRF have been described in the literature for the treatment of acne scarring [ , ]. While they can offer significant improvements in acne scarring, the longer recovery times and higher risk of complications with ablative lasers limit their use [ , ]. In contrast, NAFL and MNRF are less aggressive, offering enhanced patient tolerance, shorter recovery periods, and a more favorable safety profile, making them increasingly popular in clinical practice.
This article aims to explore the therapeutic potential of combining NAFL and MNRF in the treatment of acne scarring. We will review the clinical outcomes associated with this combination therapy, discuss the benefits and risks, and offer practical considerations for integrating these treatments into real-world clinical practice. Ultimately, we seek to provide an evidence-based framework to optimize therapeutic outcomes, improving both the aesthetic results and the quality-of-life for individuals affected by this common and often emotionally burdensome condition.
Background: monotherapy efficacy
Non-ablative Fractional Laser
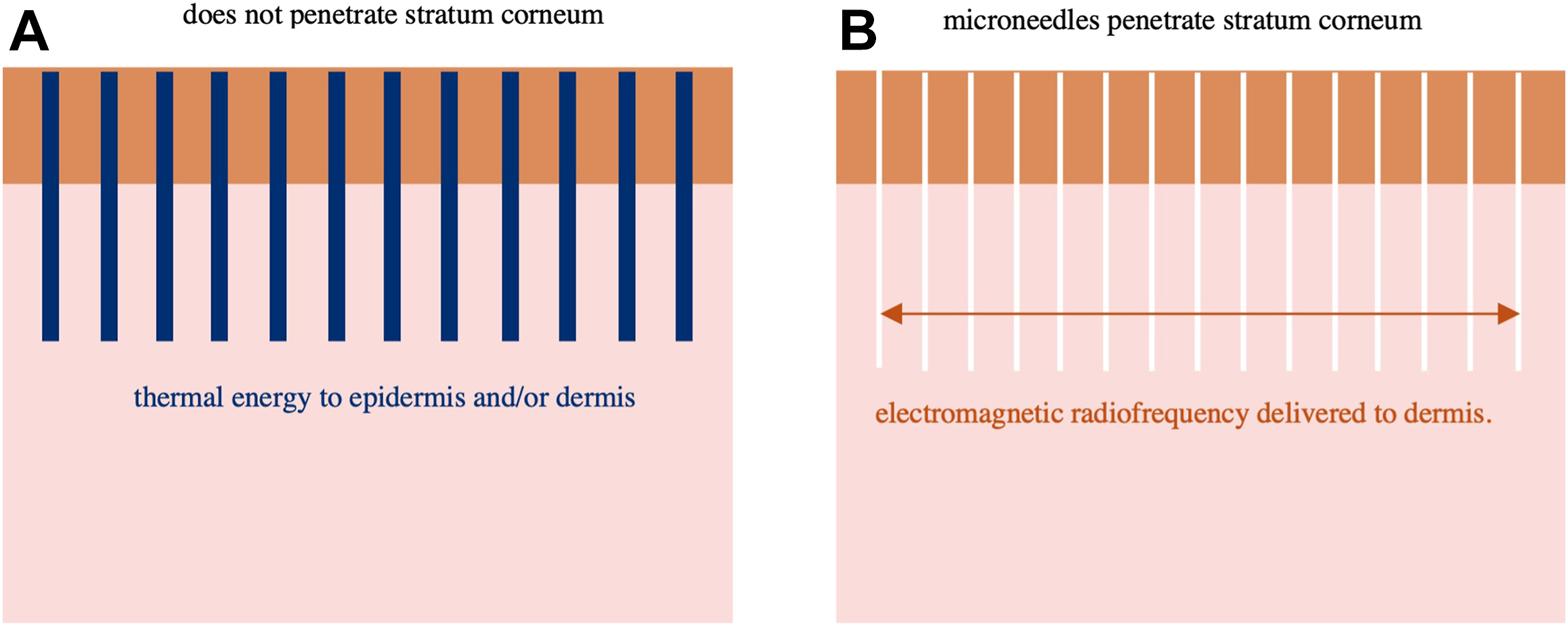
NAFL operate through the principle of fractional photothermolysis, in which microscopic columns of thermal energy are delivered to the epidermis and/or dermis with preservation of the stratum corneum [ ]. This stimulates fibroblasts, leading to neocollagenesis and neoelastogenesis ( Fig. 3 A ). The depth and density of the laser’s thermal columns can be adjusted, providing clinicians with precise control over energy delivery to the dermis.
Extensive research supports the efficacy of NAFL in improving acne scarring [ ].
- •
Alster and colleagues [ ] demonstrated a 51% to 71% improvement in acne scarring after 3 monthly treatments with a 1550-nm erbium-doped fiber NAFL.
- •
In a randomized controlled trial, Hedelund and colleagues [ ] showed a significant improvement in acne scarring for patients after 3 monthly treatments with a 1540-nm NAFL ( P = .0313).
- •
Bencini and colleagues [ ] evaluated 87 patients with moderate-to-severe acne scarring, treating them with 6 sessions of a 1540-nm erbium glass fiber NAFL at 3-week intervals. Six months post-treatment, 92% (80/87) of patients demonstrated marked improvement, while 8% (7/87) of patients showed moderate improvement.
These findings have been corroborated in subsequent studies, solidifying NAFL as an efficacious treatment of acne scarring [ ].
Radiofrequency Microneedling
MNRF is a procedure in which microneedles penetrate the epidermis with minimal damage and deliver controlled electromagnetic radiation to the dermis, creating thermal injuries in the dermis [ , ]. This activates fibroblasts, stimulates the release of growth factors, and promotes both neocollagenesis and neoelastogenesis ( Fig. 3 B) [ , , ]. The ability to adjust the depth of needle penetration allows for tailored treatments, enabling clinicians to target various layers of the dermis depending the severity and type of scarring [ ].
Similarly to NAFL, MNRF has been shown to be effective for the treatment of acne scarring.
- •
Cho and colleagues evaluated the efficacy of bipolar MNRF in patients with mild to moderate acne scarring, observing improvement in over 70% of patients after 2 monthly treatments ( P <.05) [ ].
- •
A retrospective study by Chandrashekar and colleagues investigated the efficacy of MNRF in patients with acne scarring with 4 sessions at 6-week intervals [ ]. Notably, 85.71% of patients with Grade 4 scars showed an improvement of 2 grades, 80.64% of patients with Grade 4 and Grade 3 scars improved by 2 grades, and 76.47% of patients with Grade 3 scars improved by 2 grades.
Further studies have reinforced these findings, demonstrating MNRF as an effective modality for acne scarring [ , , ].
Non-ablative Fractional Laser Monotherapy Versus Microneedling with Radiofrequency Monotherapy
When comparing NAFL and MNRF head-to-head for the treatment of acne scarring, studies have demonstrated comparable efficacy between the 2 modalities:
- •
Rongsaard & Rummaneethorn conducted a randomized, split-face trial involving 20 patients, treating one side of the face with a 1550-nm NAFL and the other with MNRF at 4-week intervals for 3 sessions. Both groups showed significant improvements on a grading scale ranging from 0 to 4, with NAFL yielding a mean improvement of 2.86 ± 0.42 on the grading scale ( P <.001) and MNRF achieving a mean improvement of 2.70 ± 0.37 ( P <.001). However, there was no statistically significant difference in efficacy between the 2 treatment modalities [ ].
- •
Chae and colleagues led a trial in which 40 patients were randomized to receive either NAFL or MNRF at 4-week intervals for 3 sessions. Acne scarring was graded using the échelle d’évaluation clinique des cicatrices d’acné (ECCA) score, showing a mean improvement of 25% in the NAFL group ( P <.01) and 18.6% in the MNRF ( P <.01). While NAFL demonstrated a larger reduction in scar severity, the difference between the groups was not significant ( P >.05). When evaluating an improvement by scar type subgroups, there was not a significant difference between the 2 treatments ( P >.05) [ ].
Surgical technique
Pre-operative Planning
Ideal candidates for combination treatment with NAFL and MNRF are those with moderate to severe acne scarring [ , ]. As with any procedure, pre-treatment consultation is crucial and should include a thorough discussion regarding treatment protocol, risks, benefits, alternatives, and expected results. It is important to counsel patients regarding realistic expectations for improvement, and that multiple treatment sessions are often needed, especially for deeper atrophic acne scars. Patients should also be aware of potential downtime prior to scheduling the procedure. After consultation, patients should provide written informed consent. Prior to treatment, baseline photographs should be taken of the treatment area (direct anterior view, 45-degree oblique views, and 90-degree side views), and photos should be repeated at each visit to monitor improvement. Typically, NAFL and MNRF are performed together at the same visit, but for patients who have a risk of prolonged healing or are prone to hyperpigmentation, then these 2 treatments may be spaced out and alternated at 2 to 4 week intervals, though patients should be aware that this approach will result in a longer total treatment time and slower or reduced improvement [ ].
In our practice, we use the 1550-nm erbium doped-fiber laser (Fraxel, Solta Medical; Bothwell, WA) for NAFL treatment. For MNRF, we employ Legend Pro (Lumenis Be Ltd; Yokneam, Israel), the Morpheus 8 (InMode; Irvine, CA), and the Genius (Lutronic; Billerica, MA). For patients with higher Fitzpatrick skin types, use of insulated tips and bipolar electrodes will prevent epidermal heating and protect against hyperpigmentation. We recommend treating first with NAFL followed by MNRF- we employ laser settings of 50 to 70 J/cm 2 , treatment level 8, with 8 passes, with decreased energy, density, and/or treatment level for skin of color. MNRF settings are detailed further below in the Procedural Approach section.
Preparation and Patient Positioning
Prior to treatment, the provider should apply an even layer of topical numbing ointment (30% compounded lidocaine ointment) for 45 to 60 minutes to the treatment area to ensure patient comfort. The skin should then be cleansed with gauze followed by alcohol to degrease and sanitize the skin. The patient should be positioned supine, and each device should be positioned close enough for the hand piece to easily reach all areas to be treated. Standard laser safety protocols should be employed, including appropriate signage on the examination room door and eye protection for both patient and clinician. Prior to MNRF, clinician should also confirm there is no pacemaker in place.
Procedural Approach
For NAFL treatment, we recommend treating the whole face to avoid a treatment demarcation line, while MNRF can be limited to the area of scarring. For NAFL, we treat by unit of the face to allow for clinician comfort and accuracy, starting with the cheeks, followed by the chin and upper lip, nose, and ending with the forehead. In each sub-region, the laser handpiece should be directed along the skin in a single back and forth motion, with 50% overlap between each row; this pattern should be repeated perpendicularly in the same treatment sub-region, to yield a total of 8 passes. Clinical endpoint is mild erythema and edema.
For MNRF, for Legend Pro, we pretreat with pure glycerin and pre-heat the target area with the TriPollar tip to a temperature of 100 to 102°F. The area is then treated with a single pass with a 7x7mm, 0.2 mm depth trifractional tip, followed by a second pass with a 6x6mm, 1.0 mm depth tip. Of note, given the pre-heating in the protocol, we do not recommend use of topical numbing if the Legend Pro is being used given risk of burn due to decreased temperature sensation. For the Morpheus 8 device, we use the 24-pin tip and perform 3 passes with decreased depth and energy with each subsequent pass, noted below ( Table 1 ). For the Genius device, we perform 2 passes using the M49 tip, with passes and energy noted below ( Table 2 ). For patients with Fitzpatrick skin types V and VI, energy settings should be decreased by at least 25%.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


