Closed Nasal Fracture Correction
Benjamin C. Wood
DEFINITION
Nasal bone fracture is the most common type of facial fracture.1
The combination of the central positioning and anterior projection of the nose, with the delicate nature of the thin nasal bones, increases the risk of fracture from traumatic injury.
ANATOMY
The pyramidal shape of the nose is composed of skeletal and cartilaginous structural components supporting the overlying skin and soft tissue (FIG 1).
The bony structure of the nose is composed of the paired, wedge-shaped nasal bones in the midline, which articulate with the frontal process of the maxilla, the nasal process of the frontal bone, and the ethmoid and vomer.
The cartilage structures of the nose include the paired upper lateral cartilages and lower lateral cartilages and the septum, which is composed primarily of the quadrangular cartilage.
PATHOGENESIS
The most common cause of nasal fractures is blunt trauma, typically due to motor vehicle accidents, physical altercations, or sports-related injuries.2
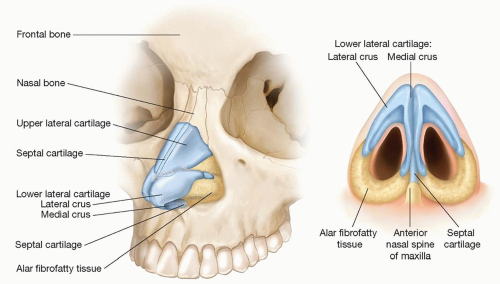 FIG 1 • Nasal structural anatomy. |
PATIENT HISTORY AND PHYSICAL FINDINGS
Delineate pertinent patient history, including mechanism of injury, time since injury, and any pre-existing nasal deformity or previous nasal surgery.
Establish any prior history of nasal breathing difficulty, obstruction, or sleep apnea, including use of allergy medications, nasal sprays, or inhalers.
External examination should focus on the severity of nasal deformity, lacerations, epistaxis, cerebrospinal fluid drainage, and pain or step-off on palpation.
It is important to determine whether there is suspicion of a naso-orbital ethmoid (NOE) fracture on examination, which may warrant further evaluation with imaging.
Internal examination using a nasal speculum to identify any mucosal lacerations, septal deviation, or the presence of a septal hematoma.
Vasoconstrictive agents and topical anesthetic should be used to control bleeding and facilitate a proper internal nasal examination.
Pediatric patients less frequently fracture the nasal bones but are more susceptible to failure to identify a septal hematoma on examination.3
IMAGING
Nasal fractures are generally a clinical diagnosis, so radiographic imaging is of minimal utility unless there is suspicion of a more complex facial fracture pattern.
NONOPERATIVE MANAGEMENT
Patients with minimal nasal symmetry distortion and patent nasal airways may be managed expectantly with observation and reassessment following resolution of soft tissue edema.
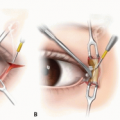
SURGICAL MANAGEMENT
The timing of surgical management is dependent on the time since the injury occurred.
Patients presenting within hours of the injury before substantial edema develops may be amenable to immediate closed nasal reduction.
Patients presenting more than 3 or 4 hours after injury should have operative intervention deferred until sufficient time has passed to allow for resolution of edema to facilitate full visualization of the deformity.
The decision for closed vs open nasal reduction depends on the severity of the injury.
Simple, unilateral or bilateral, fractures are generally amenable to closed nasal reduction.
Comminuted, closed or open, fractures may be better addressed with an open reduction.
Septal hematomas always require immediate evaluation to avoid septal cartilage resorption and formation of a secondary nasal deformity.4Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree