Introduction
Head and neck reconstruction presents unique challenges to the reconstructive surgeon. Because of the visibility of this region, defects are often difficult to conceal and the demands on the surgeon’s reconstructive skills are greater than they are elsewhere in the body where cosmesis may be less vital and function less specialized. The head and neck area includes both static and dynamic structures and contains organs of special function such as the nose, the ears, the lips, and the orbital contents, including the eyelids.
The bony skeleton of the head and neck is related to structure and load, as are bony structures elsewhere in the body. In addition, however, certain structures such as the mandible have a very specialized function and therefore have unique reconstructive requirements. The soft tissues of the face are also unique and provide external cover, internal mucosa, and facial animation. The external cover provides a barrier, which in some cases is specialized such as the hair-bearing skin of the scalp. In addition to the external skin cover, it is frequently necessary to replace the mucosa. The facial muscles provide a unique and very delicate function for facial animation and are innervated by the complex facial nerve. This nerve is sometimes sacrificed to execute an effective tumor ablation and the loss of facial nerve function will further complicate the reconstruction. Not infrequently all of the above elements are involved in the reconstruction. For all of the aforementioned reasons, a thorough knowledge of the anatomy of this region is imperative, not only for the ablative surgeon in cancer cases but also for the reconstructive surgeon, so that the best possible reconstruction can be achieved, to optimally restore the cosmetic and functional elements of the defect.
Anatomy of the Head and Neck
The anatomy of the head and neck is complex. The calvarium provides protection for the underlying brain and is covered with hair-bearing soft tissue. The skin of the rest of the face is intimately related to the underlying musculature and movement of this multifaceted unit not only gives the skin its unique appearance, with multiple lines and wrinkles, but also is responsible for a significant aspect of how we communicate. For this reason, replacing large segments of facial skin with skin from elsewhere in the body often results not only in a color mismatch but also a texture and movement imbalance. Within the head and neck region, there are several structures with specialized function and anatomic distinctiveness, including the eyelids, the nose, the lips, and the ears. All these structures are particularly difficult to replicate and pose significant challenges. Within the head and neck, there are also mucosa-lined cavities, which all lead into the aerodigestive tract. Within the mouth, there is another even more specialized organ, the tongue, which is vital to the functions of speech and swallowing.
Anatomy of the Facial Skeleton
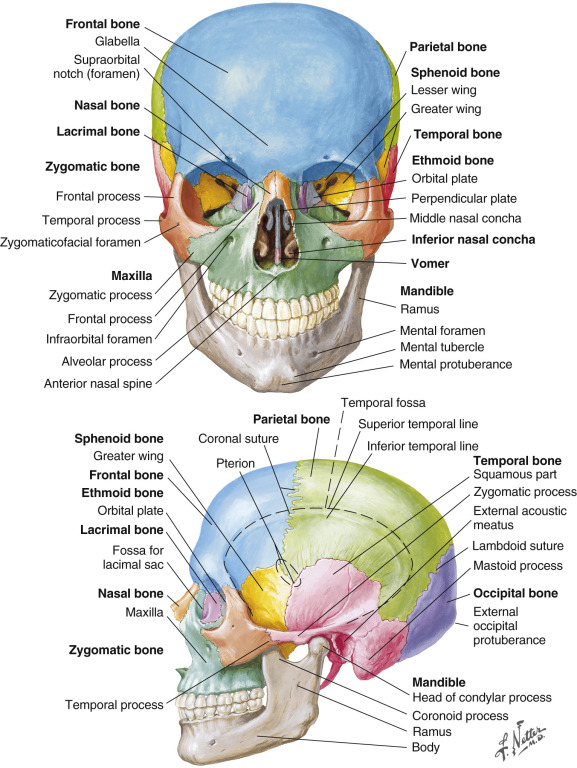
The facial skeleton is complex, made up of several individual bony structures, articulated in a complex manner ( Fig. 10.1 ). The calvarium, consists of frontal, parietal, temporal and occipital bones which protects the brain. The cranial bones in turn articulate with the skull base (sphenoid bone) and midfacial skeleton consisting of the maxilla, ethmoid, lacrimal, zygomatic, nasal, palatine, nasal concha, and vomer. The facial skeleton provides protection of delicate structures such as the eye, and also provides protective passage for some vital structures such as the facial nerve, which passes through the temporal bone. Other clinically important nerves to be considered during craniofacial surgical exposures include the supraorbital and supratrochlear nerves (V1), the infraorbital nerve (V2), the inferior alveolar nerve (V3), and its terminal branch, the mental nerve. The supraorbital nerve exits the frontal bone through a foramen or a notch. In elevation of a bicoronal flap or a paramedian forehead flap, transition to subperiosteal dissection 1–2 cm above the supraorbital rim avoids injury to the supraorbital nerve or supratrochlear neovascular bundle. The infraorbital nerve exits the infraorbital foramen 6–11 mm below the inferior orbital rim at the midpupillary line. The mental nerve exits the metal foramen in the body of mandible between the root apices of the mandibular first and second premolars. The ethmoid, sphenoid and maxillary bones, house the intricate system of air cells and sinuses that contribute to humidification of inspired air, and resonance for voice reproduction. The mandible not only provides the structure that defines the appearance of the lower face but, combined with its sister bone, the maxilla, provide a housing for the dentition and defines the confines of the oral cavity and all that it contains. Finally, the facial skeleton also provides the framework from which the facial muscles take origin.
The Fascia of the Head and Neck
An understanding of the fascia of the head and neck is paramount ( Fig. 10.2 ), as they provide important landmarks for important anatomic structures during surgical exposures such as the facial artery, facial nerve, superficial temporal vessels, and other recipient vessels in head and neck reconstruction. In general, the two main fascial layers investing the head and neck are the superficial and deep fascial layers, which are interconnected as they envelop the various muscles. The superficial fascia is an anatomically continuous layer that is named differently according to the zone it covers. Most cephalad, the galea aponeurotica, is a fascial expansion that connects the paired frontalis and occipitalis muscles and runs in an anteroposterior direction over the vertex of the head. The lateral extension of the galea aponeurotica is continuous with the temporoparietal fascia (TPF), also known as the superficial temporal fascia, lateral to the superior temporal line. The TPF is continuous with the galea superiorly, the frontalis muscle anteriorly, and the SMAS inferiorly. Inconsistent nomenclature of the temporal fascia has generated confusion in its anatomic descriptions.
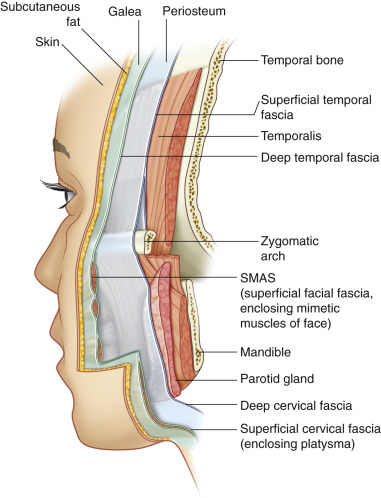
The TPF is a thin translucent layer underneath the skin and subcutaneous tissue of the temple. In the temple region, nine anatomic layers exist, including – from superficial to deep: the skin; the subcutaneous tissue; the temporoparietal fascia (or superficial temporal fascia); the loose areolar layer (or innominate fascia); the superficial layer of the deep temporal fascia; the superficial temporal fat pad; the deep layer of the deep temporal fascia; the deep temporal fat pad; and the temporalis muscle. The superficial temporal artery and vein run within the TPF and provide the vascular pedicle to the temporoparietal fascia flap. After exiting the parotid gland, the frontal branch of the facial nerve crosses over the zygomatic arch within the innominate fascia, where it remains for a distance of 1.5–3.0 cm above the superior border of the arch. After that transition point, the nerve becomes more superficial and travels on the undersurface of the TPF (superficial temporal fascia) until reaching the frontalis muscle. Dissection above the zygomatic arch and lateral to the eyebrow should be carried on the temporalis muscle fascia, deeper to the TPF, to avoid injury to the frontal branch. The nerve can then be reflected along with the TPF and protected. The temporoparietal fascia is distinct from the temporalis muscle fascia, which is a deeper fascia to the TPF, has a sturdier consistency, and a glistening white color. The temporalis muscle fascia covers the temporalis muscle. The temporalis muscle fascia (also known as the deep temporal fascia) splits above the zygomatic arch into two leaflets: the superficial layer of the deep temporal fascia, which is adherent to the lateral zygomatic arch periosteum, and the deep layer of the deep temporal fascia, which runs medial (deeper) to the zygomatic arch ( Fig. 10.2 ). The temporal fat pad is located between the superficial and deep layers of the deep temporal fascia. The buccal fat pad is located deeper to the deep layer of the deep temporal fascia. Caudally, the superficial temporal fascia is continuous with the superficial musculoaponeurotic system (SMAS). The SMAS is encountered deeper to the skin and subcutaneous fat. The SMAS envelops the muscles of facial expression. The parotidomasseteric fascia is a deeper facial layer that is adherent to the parotid capsule and is continuous with the superficial layer of the deep temporal fascia below the zygomatic arch. The facial nerve branches exit the parotid gland deeper to the parotidomasseteric fascia below the zygomatic arch and then pierce this fascia and become more superficial as they innervate the respective mimetic muscles. The fascia in the neck is similarly organized into the superficial and deep fascial layers. The superficial cervical fascia envelops the platysma muscle and is found closely associated to the subcutaneous fat of the neck. The superficial cervical fascia and the platysma muscle are continuous with the SMAS of the face. The deep cervical fascia is organized concentrically of the superficial layer of the deep cervical fascia (SLDCF), the middle layer of the deep cervical fascia (pre-tracheal fascia), and the deep layer of the deep cervical fascia (prevertebral fascia). The SLDCF envelops the sternocleidomastoid muscles, trapezius muscles, and attaches onto the cervical spinous processes. The SLDCF is an extension of the parotidomasseteric fascia in the neck. It is an important fascial layer, as the marginal mandibular branch of the facial nerve is found within or deep to the SLDCF. The facial artery and vein are found deeper to this plane. Once the platysma muscle has been divided, care should be taken when exposing the facial vessels by retracting and protecting the marginal mandibular branch of the facial nerve along with the SLDCF. The marginal mandibular branch runs superficial to the facial artery and vein at the premasseteric notch of the mandible.
Anatomy of the Facial Musculature
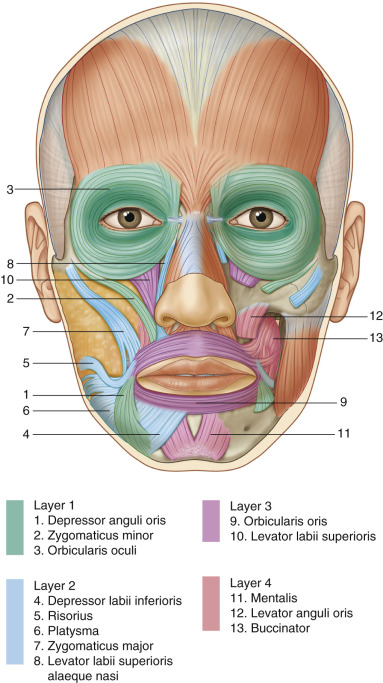
The facial muscles are complex. They consist of the muscles of facial expression as well as the muscles of mastication. In general, the muscles of facial expression are thin ribbons of muscle arranged in a radial pattern around the sphincters of the eye (orbicularis oculi) and the mouth (orbicularis oris). They consist of 17 paired muscles that give the human face the ability to move in multiple vectors or combinations of vectors and, as already mentioned, provide a significant contribution to non-verbal communication. The muscles of facial expression glide over an intricate system of fat pads in the face. Superiorly, the paired frontalis muscles insert into the galea aponeurotica, which forms an intermediate aponeurosis with the paired occipitalis muscles. Lateral to the superior temporal line, the temporoparietal fascia is continuous with the galea. The mimetic facial muscles originate from the facial skeleton and insert into the skin that they animate. These muscles are innervated by the facial nerve and, as a general rule, the facial nerve branches enter the deep surfaces of these muscles, except for the mentalis, levator anguli oris, and buccinator. They are arranged in four layers ( Fig. 10.3 ). Layer 1 (the most superficial) includes the depressor anguli oris, zygomaticus minor, and orbicularis oculi. Layer 2 includes the depressor labii inferioris, risorius, platysma, zygomaticus major, and levator labii superioris alaeque nasi. Layer 3 includes the orbicularis oris and levator labii superioris. Layer 4 (the deepest layer) includes the mentalis, levator anguli oris, and buccinator. Layer 4 muscles are innervated by the facial nerve on their superficial surfaces. The SMAS layer, which invests the mimetic muscles, is continuous inferiorly with the platysma. The buccinator, also innervated by the facial nerve, and strictly speaking not a masticatory muscle, assists in chewing, by keeping the food bolus within the occlusal plane of the molars. Posteriorly, it inserts into the pterygomandibular raphe, which separates it from the superior pharyngeal constrictor posteriorly. It is used in whistling and smiling, and in the neonate, is the muscle that assists suckling. The true muscles of mastication consist of the paired temporalis, masseter and the pterygoid muscles (medial and lateral). Unlike the muscles of facial expression, which are all innervated by the facial nerve (CN VII), the four muscles of mastication are all innervated by the mandibular branch of the trigeminal nerve (CN V). The temporalis muscle arises from the superior temporal line and the temporal fossa, its fan-shaped origin coalesces inferiorly as its fibers pass medially to the zygomatic arch to insert onto the coronoid process of the mandible and anterior border of the ramus. This muscle is supplied by branches the internal maxillary artery, namely the anterior and posterior deep temporal arteries, which enter the muscle on its deep surface anterior and posterior to the cornoid process, respectively. An additional arterial supply is the middle temporal artery, a branch of the superficial temporal artery, which supplies the deep temporalis muscle fascia. This muscle has several applications for local reconstruction of defects of the cheek, orbit and in facial reanimation. A powerful mandibular elevator, the masseter muscle arises from the lower border of the zygoma and the most anterior fibers arise from the zygomatic process of the maxilla and inserts into the lateral surface of the mandible. The masseter muscle is innervated by the masseteric nerve, a branch of V3, which reaches the deep surface of the muscle through the coronoid notch. The blood supply to the masseter is furnished by the masseteric artery, a branch of the internal maxillary artery. Individuals of these muscles are expendable so the nerve to the masseter can be used to innervate a free functional muscle transfer for the treatment of facial paralysis.
Arterial Anatomy of the Head and Neck
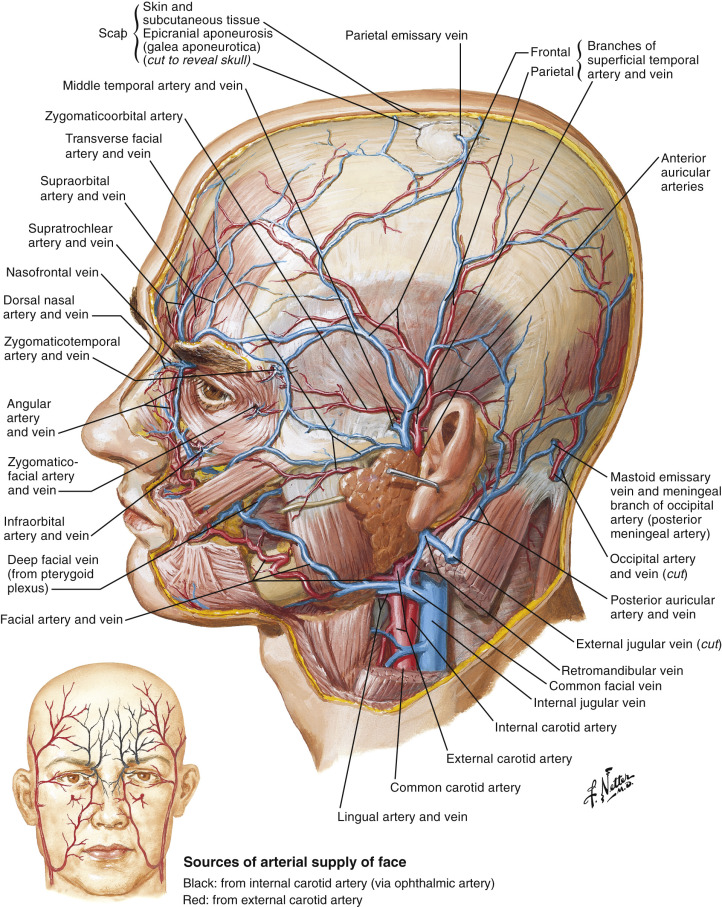
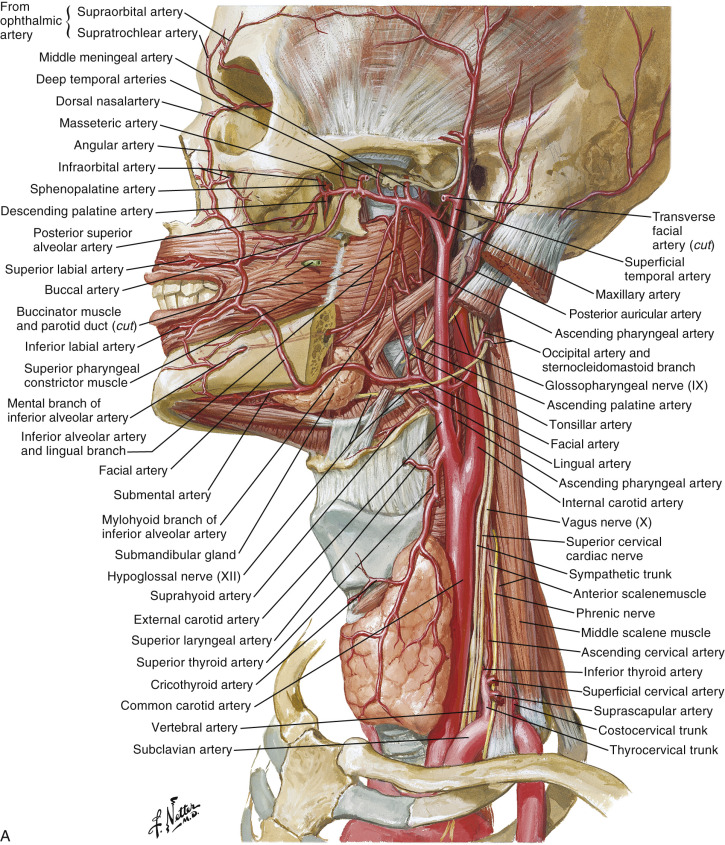
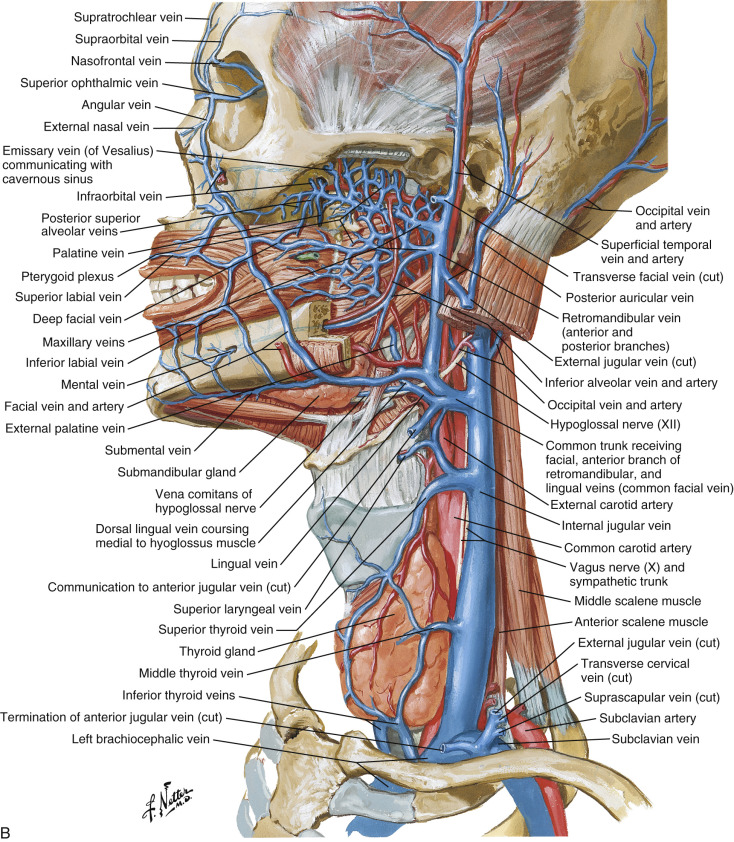
The head and neck is one of the most highly vascularized regions in the body ( Figs 10.4 and 10.5 ). The external carotid arterial system supplies most of the skin of the head, with the exception of a central triangle that includes the eyes, the bridge of the nose, and a central portion of the forehead. This latter area is vascularized by the ophthalmic branch of the internal carotid artery. The superficial temporal, posterior auricular, and occipital arteries supply the scalp. Most of the external carotid branches are commonly used for microvascular anastomosis, however, the four most commonly used recipient vessels for head and neck reconstruction are: the facial artery; the superficial temporal artery; the superior thyroid artery, which are branches of the external carotid artery; and the transverse cervical artery, a branch of the thyrocervical trunk.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


