Introduction
The reconstructive microsurgeon is often consulted for management of lower extremity bone and soft tissue defects. Defects can arise from multiple causes, including trauma, oncologic resection, infection, or pre-existing vascular disease. By far, trauma is the most common etiology for lower extremity defects that require microsurgical reconstruction. This chapter delineates clinically relevant anatomy in the lower extremity and provides anatomic and technical descriptions of exposing recipient vessels in this region.
Anatomy of the Thigh
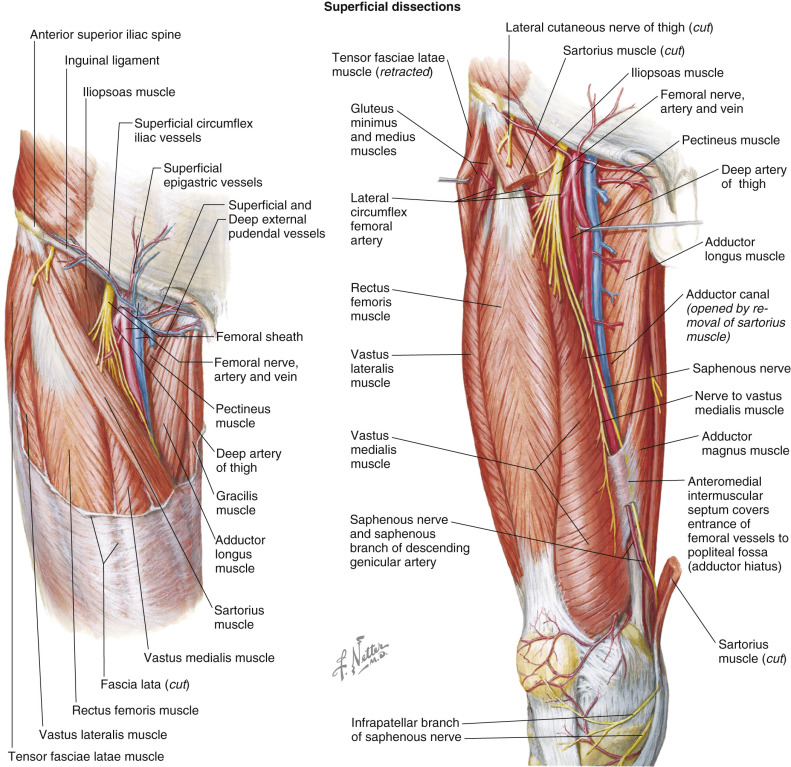
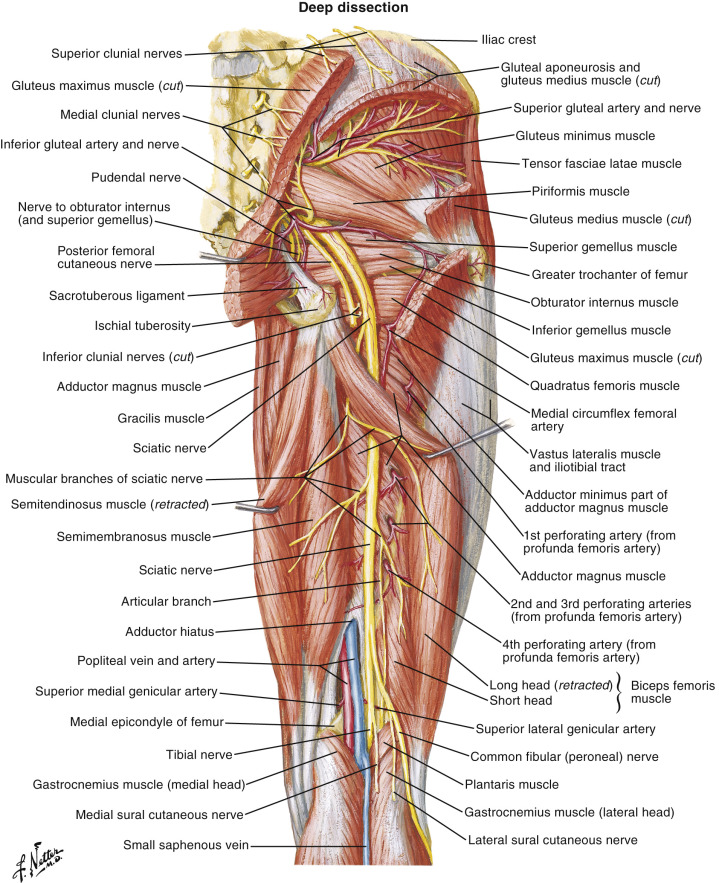
Thigh muscles are divided into anterior, medial, and posterior compartments (see Fig. 13.1 ). Within the anterior compartment are the sartorius and quadriceps muscles, which include the rectus femoris (see Figs 13.1 and 13.2 ), vastus lateralis, vastus medialis, and vastus intermedius. The femoral nerve provides innervation to these muscles. The psoas major and iliacus muscles are also found in the upper part of this compartment. The rectus femoris crosses the hip joint and knee joint, whereas the vastus muscles originate on the femur and cross the knee joint only. The posterior compartment contains the hamstring muscles including the semitendinosus, semimembranosus and biceps femoris, which are all innervated by the sciatic nerve. (see Fig. 13.3 )
The medial compartment contains the gracilis, pectineus, adductor longus, adductor brevis, adductor magnus, and obturator externus. The obturator nerve supplies innervation to all these muscles except the pectineus (femoral nerve) and part of the adductor magnus (sciatic nerve).
Nerves
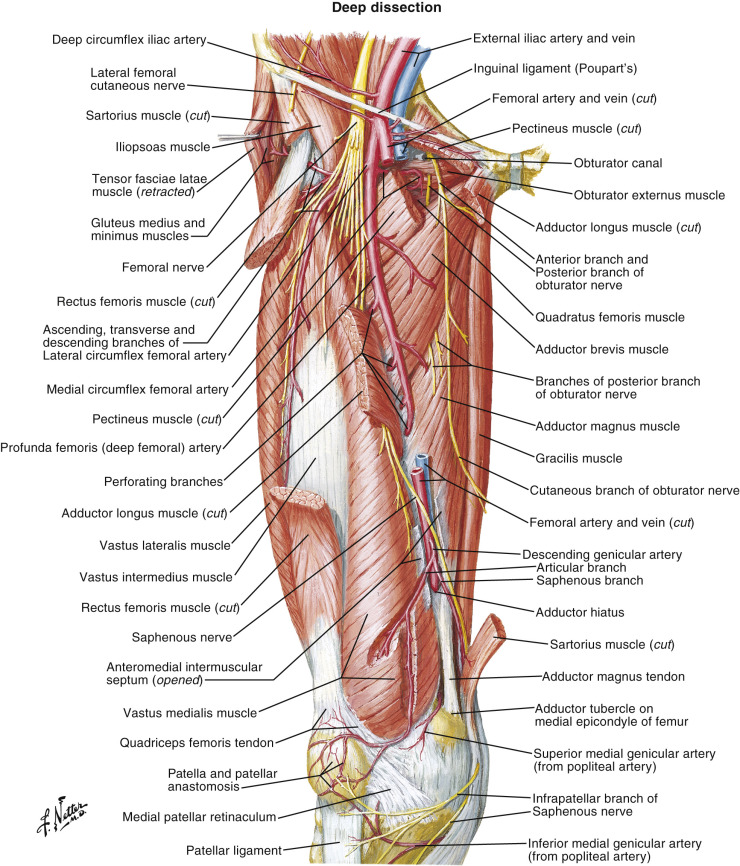
Three main nerves traverse the thigh, the femoral nerve (L2–L4) (see Fig. 13.1 ), the sciatic nerve (L4–S3), and the obturator nerve (L2–L4) (see Fig. 13.3 ). The femoral nerve passes through the anterior compartment; the obturator through the medial compartment; and the sciatic through the posterior compartment. The femoral nerve above the inguinal ligament gives off branches that supply the iliacus and psoas muscles, then below, the inguinal ligament gives off branches that supply the anterior compartment muscles. Below the ligament, the femoral nerve also gives off an anterior cutaneous branch supplying the anterior thigh and knee skin, and the saphenous nerve which supplies the medial side of the leg and foot. The obturator nerve passes through the obturator canal into the medial compartment and divides into a posterior and anterior branch. The anterior branch supplies innervation to the adductor longus, gracilis, adductor brevis and the skin on the medial aspect of the thigh. The sciatic nerve supplies all the muscles of the posterior compartment and continues on to the knee, dividing into the tibial and common peroneal nerve.
The lateral femoral cutaneous nerve (L2–L3) is a direct branch of the lumbar plexus and enters the thigh deep to the lateral end of the inguinal ligament. It travels under the tensor fascia lata for ~10 cm before rising through it and dividing into anterior and posterior branches that supply the skin of the anterolateral thigh. It is found in the deep subcutaneous tissue just above the fascia. The motor branch to vastus lateralis muscle originates from the femoral nerve and accompanies the descending branch of the lateral femoral circumflex artery (LCFA) along the intermuscular septum.
Arterial Anatomy of the Thigh
Common Femoral Artery
The external iliac artery becomes the common femoral artery ( Fig. 13.3 ) as it passes underneath the inguinal ligament. In the proximal thigh, the common femoral artery passes through the femoral triangle, bounded by the sartorius laterally, the adductor longus medially, and the inguinal ligament superiorly. Just distal to the inguinal ligament, the superficial circumflex iliac artery (SCIA) and superficial inferior epigastric artery (SIEA) originate from the lateral and medial surface of the common femoral artery, respectively. Alternately, they can arise as a common trunk from the anterior surface in 48% of patients. The SCIA runs laterally approximately two fingerbreadths below and parallel to the inguinal ligament and supplies the groin flap and superficial circumflex iliac artery perforator flap. The common femoral artery divides into the superficial and deep femoral arteries. The bifurcation typically occurs 5 cm distal to the inguinal ligament.
Exposure of the Common Femoral Artery
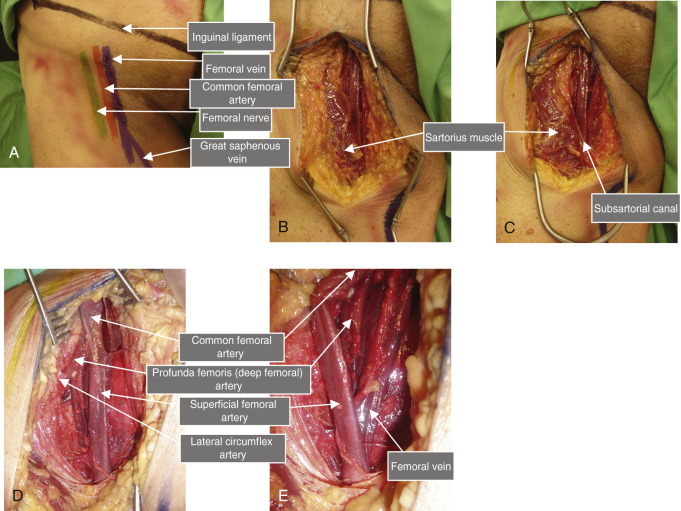
The common femoral artery ( Fig. 13.2 ) can be palpated just distal to the inguinal ligament halfway between the anterior superior iliac spine and the symphysis pubis (see Fig. 13.5 ). The femoral vein is medial and the femoral nerve is lateral to the common femoral artery. The great saphenous vein drains into the medial surface of the femoral vein. In the femoral triangle, the vessel lies superficially below the fascia of the thigh and can be approached directly.
Deep Femoral Artery (Profunda Femoris) ( Fig. 13.2 )
The lateral femoral circumflex artery is the largest branch of the deep femoral artery, arising from its lateral aspect. The vessel typically arises 1.5 cm distal to the origin of the deep femoral artery, although it branches directly from the common femoral artery in approximately 30% of patients ( Fig. 13.3 ). It courses deep to the sartorius and rectus femoris and divides into ascending, transverse, and descending branches. The ascending branch can be identified in the interval between tensor fascia lata muscle and rectus femoris, and supplies the tensor fascia lata and gluteus muscles. The descending branch runs in the interval between the rectus femoris and vastus lateralis, and is the blood supply to the anterolateral thigh flap. The rectus femoris branch is a direct branch from the descending branch of the lateral femoral circumflex artery. In 51% of patients, perforators from the rectus femoris branch pass between the rectus femoris and vastus medialis/sartorius to supply the anteromedial thigh flap.
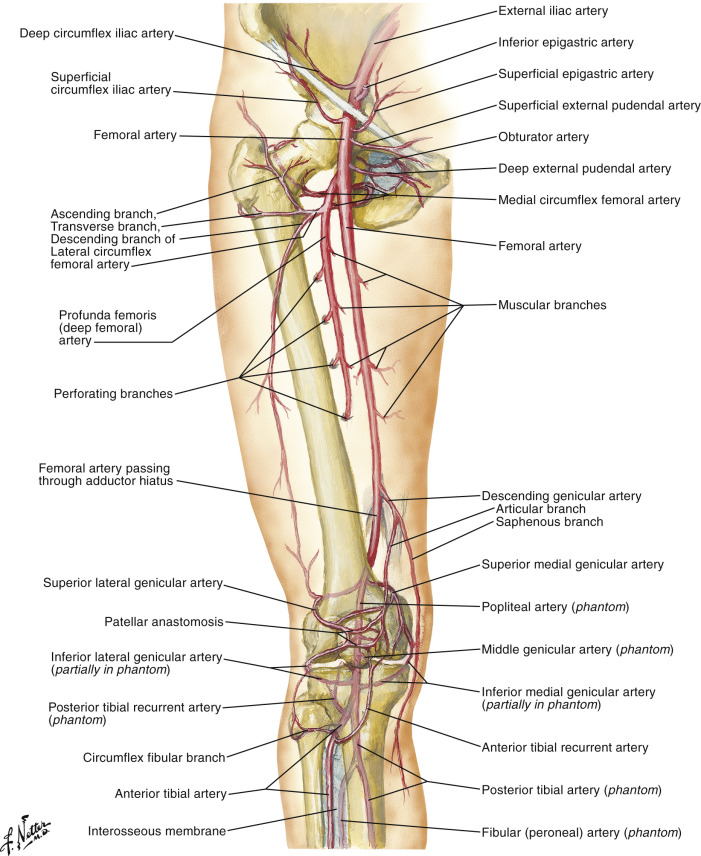
The medial femoral circumflex artery usually originates from the posteromedial aspect of the profunda femoris at the same level or close to the lateral femoral circumflex artery, but it may arise from the common femoral artery directly in 25% of patients. It divides into ascending and transverse branches. The ascending branch runs between the adductor longus and magnus and is the primary pedicle for the gracilis muscle flap.
The perforating branches of the deep femoral artery typically include three separate, numbered branches and the terminal segment of the deep femoral which is referred to as the fourth perforating branch. They perforate the adductor magnus to reach the posterior thigh ( Fig. 55.1 ).
Exposure of Branches of the Deep Femoral Artery
Branches of the deep femoral artery can be used for recipient vessels in the thigh. The descending branch of the lateral femoral circumflex vessels can be approached as if the surgeon is performing an anterolateral thigh flap ( Fig. 59.1 ). A line is drawn between the anterior superior iliac spine and the lateral border of the patella, the so-called “AP” line. An axial incision 1 cm medial to the AP line can be carried down to the rectus femoris muscle. Slightly lateral, the interval between the rectus femoris and vastus lateralis can be identified; a fat stripe is usually present at this junction. The descending branch can reliably be located within the largely avascular plane between the two muscles ( Fig. 13.2 ). A more superior incision can allow identification of the ascending branch of the lateral femoral circumflex vessels in the interval between rectus femoris and the vastus intermedius, deep to the tensor fascia lata.
Superficial Femoral Artery
The common femoral artery becomes the superficial femoral artery after the take-off of the profunda femoris ( Fig. 13.2 ). The superficial femoral artery continues through the distal femoral triangle, courses through the subsartorial canal, and ends at the hiatus of the adductor magnus, where it continues as the popliteal artery ( Fig. 13.2 ). At the entrance to the adductor hiatus (also known as Hunter’s canal), the descending genicular branch arises from the anterior portion of the superficial femoral artery ( Figs 13.4 , 13.5 , 55.1 ). This vessel runs deep to the vastus medialis muscle on the surface of the medial femoral condyle to supply the medial femoral condyle flap. The saphenous artery, a medial branch of the descending genicular artery, supplies a reliable skin island that can be included with the medial femoral condyle flap ( Fig. 13.5 ).
Exposure of the Superficial Femoral Artery and Its Branches
After giving rise to the deep femoral artery, the superficial femoral artery passes inferiorly, deep to the sartorius, and passes into the adductor canal. Distal to the femoral triangle, the superficial femoral artery can be exposed through a longitudinal thigh incision along the lateral edge of the sartorius ( Fig. 13.5 ). The incision is deepened through the muscle fascia and the lateral edge of sartorius is reflected medially; this preserves the segmental inferior-medial perforators entering the muscle. In the middle one-third of the thigh, the superficial femoral artery runs on the surface of the adductor longus. In the distal one-third, it passes through the adductor hiatus. Access requires division of the fascial connection between the adductor magnus and vastus medialis which forms the canal’s roof. End-to-side anastomosis to the superficial femoral artery requires temporary interruption to the blood supply below the knee. When present, prominent perforators including the descending genicular vessels at the adductor hiatus may be preferable to allow end-to-end anastomosis.
Anatomy of the Leg
The framework of the lower leg is composed of two long bones, the fibula and the tibia, which are arranged in parallel and connected along their length by a fibrous membrane termed the interosseous membrane These three structures together divide the leg into two anatomic sections: the anterior and posterior compartments. The anterior compartment is further divided into anterior and lateral sections separated by a thick anterior intermuscular septum. The lateral leg compartment is separated from the posterior compartment by the posterior intermuscular septum (see Fig. 13.6 ).
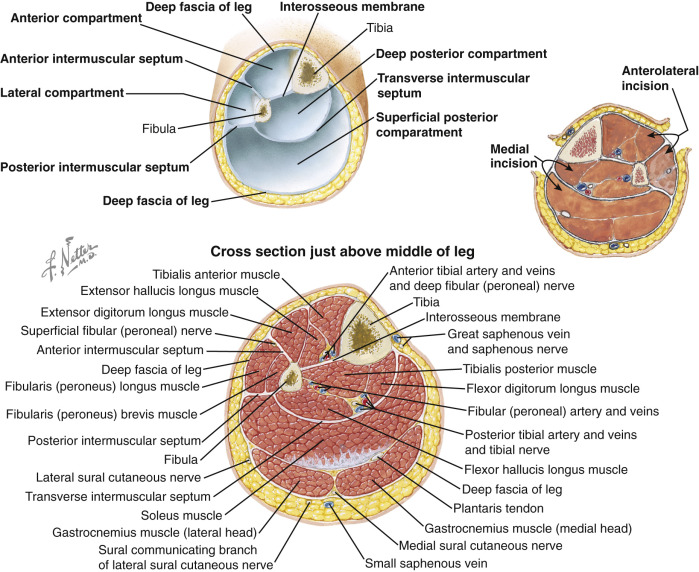
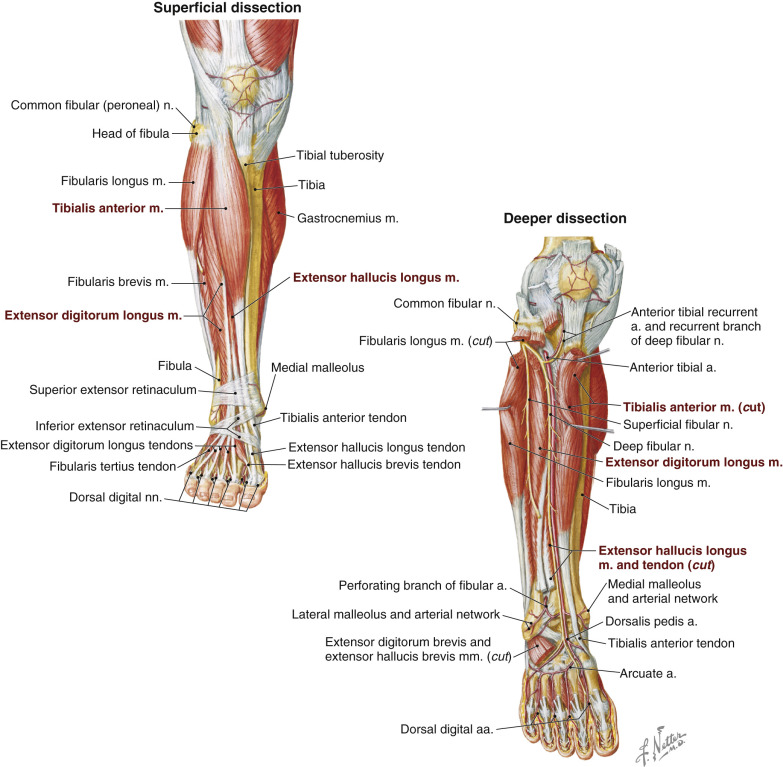
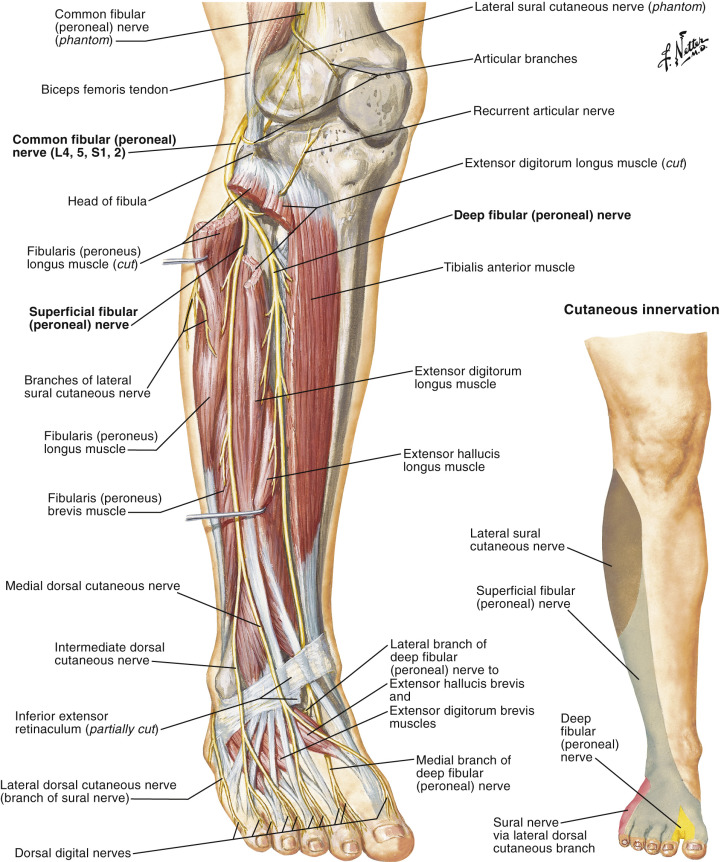
The anterior compartment has four muscles: the extensor digitorum longus, extensor hallucis longus, peroneus tertius, and tibialis anterior (see Fig. 13.7 ). These muscles are supplied by the anterior tibial vessels and are innervated by the deep peroneal nerve, all traveling deep to the muscles along the interosseous membrane (see Fig. 13.8 ).
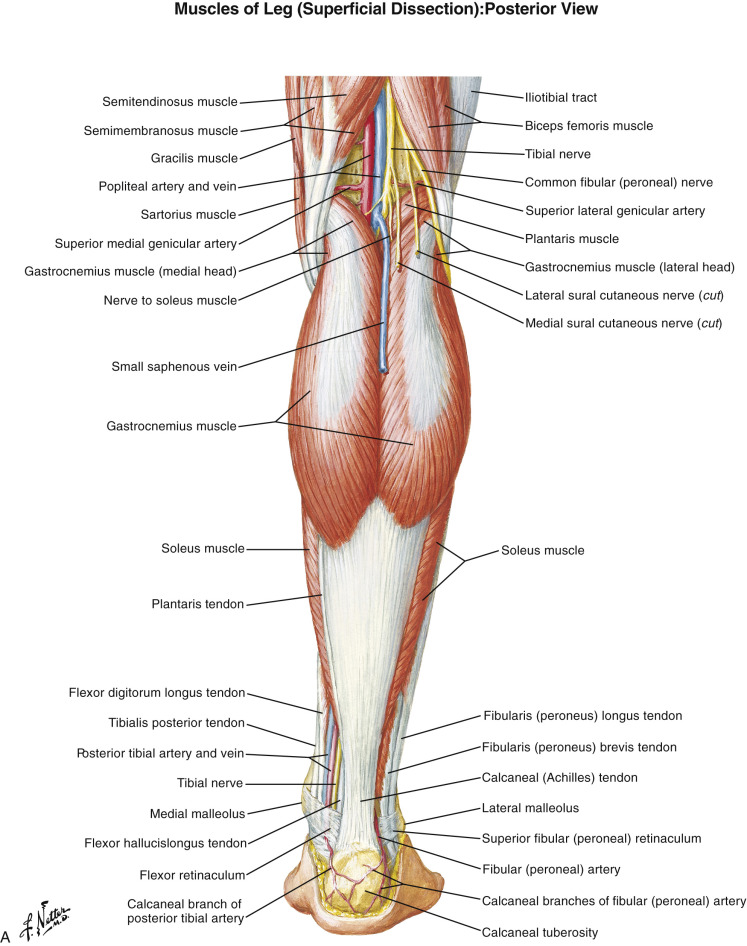
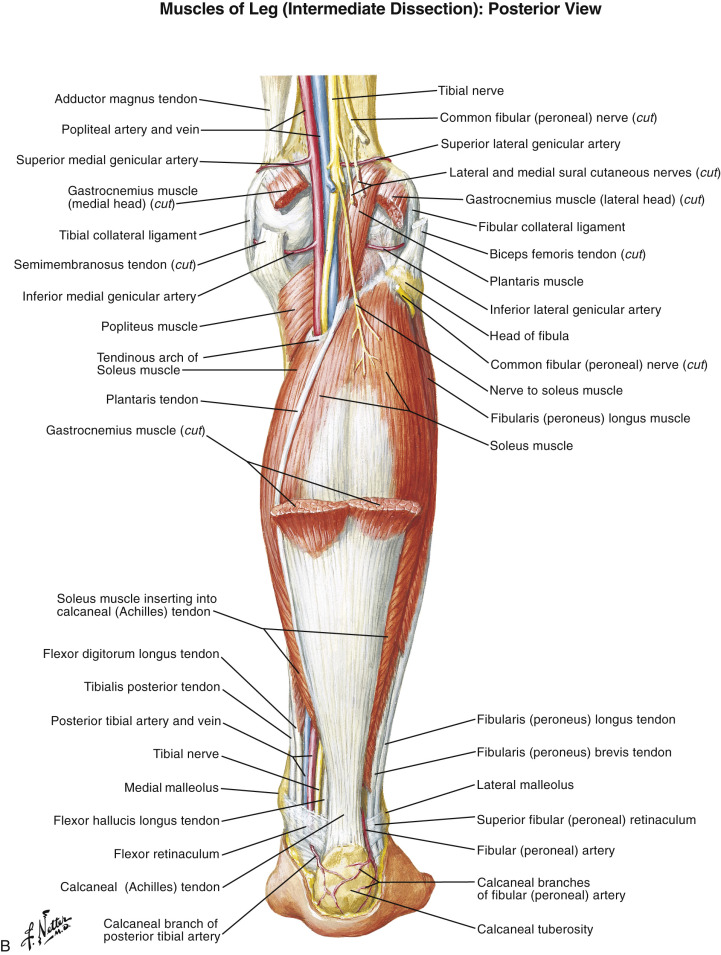
The posterior compartment is divided into superficial and deep compartments by a thin fascia termed the “transverse intermuscular septum (see Fig. 13.6 ).” Three muscles are located in the superficial compartment: the gastrocnemius, soleus, and plantaris (see Fig. 13.9 ). The gastrocnemius and plantaris originate from the femur, while the soleus originates from the posterior surface of the fibula and tibia. The gastrocnemius and soleus join together at midcalf to form the Achilles tendon, which inserts into the calcaneal bone. The plantaris is a thin, small muscle. The plantaris tendon follows the larger Achilles tendon to insert into the medial portion of the calcaneus. All these muscles flex the foot in a plantar direction (the gastrocnemius also flexes the knee) with slight inversion. The muscles are vascularized by branches from the popliteal and posterior tibial arteries and innervated by branches of the tibialis nerve from the popliteal fossa.
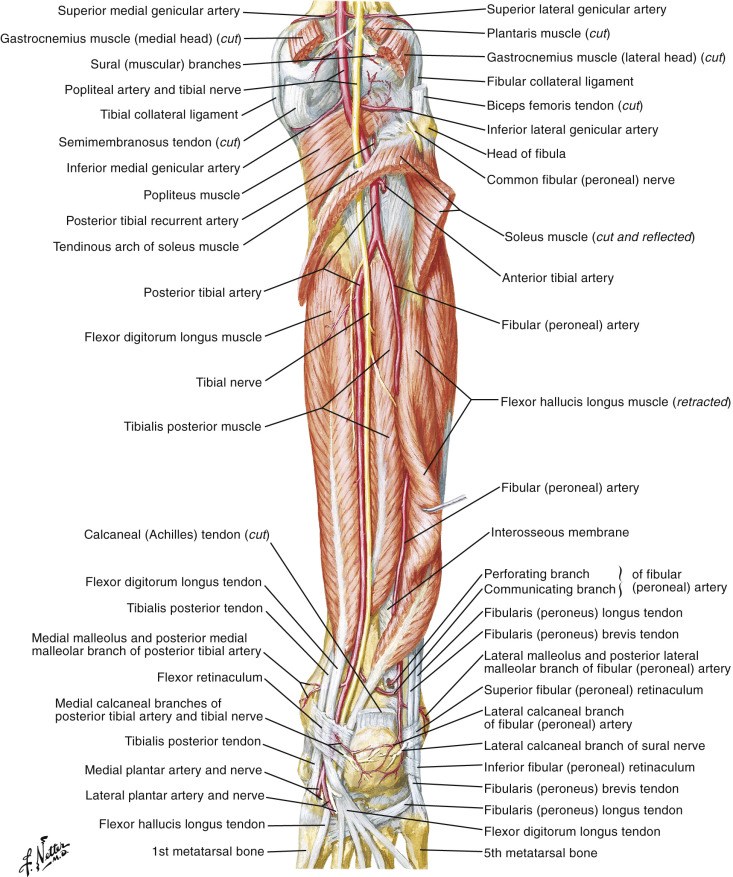
The deep posterior leg compartment contains four muscles: the popliteus, flexor digitorum longus, flexor hallucis longus, and tibialis posterior (see Figs 13.6 and 13.10 ). The popliteus performs knee flexion and medial rotation of the leg. The flexor hallucis longus muscle originates from the distal two-thirds of the fibula posteriorly, transverse intermuscular septum, and the interosseous membrane. The tibialis posterior muscle is the most deeply situated muscle in the deep posterior compartment, lying between the flexor hallucis longus and flexor digitorum longus muscles. It arises from the upper two-thirds of the fibula posteromedially, the interosseous membrane, posterolateral tibia, and transverse intermuscular septum that separates it from the soleus.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


