For videos accompanying this chapter see ExpertConsult.com . See inside cover for access details.
For videos accompanying this chapter see ExpertConsult.com . See inside cover for access details.
Embryology
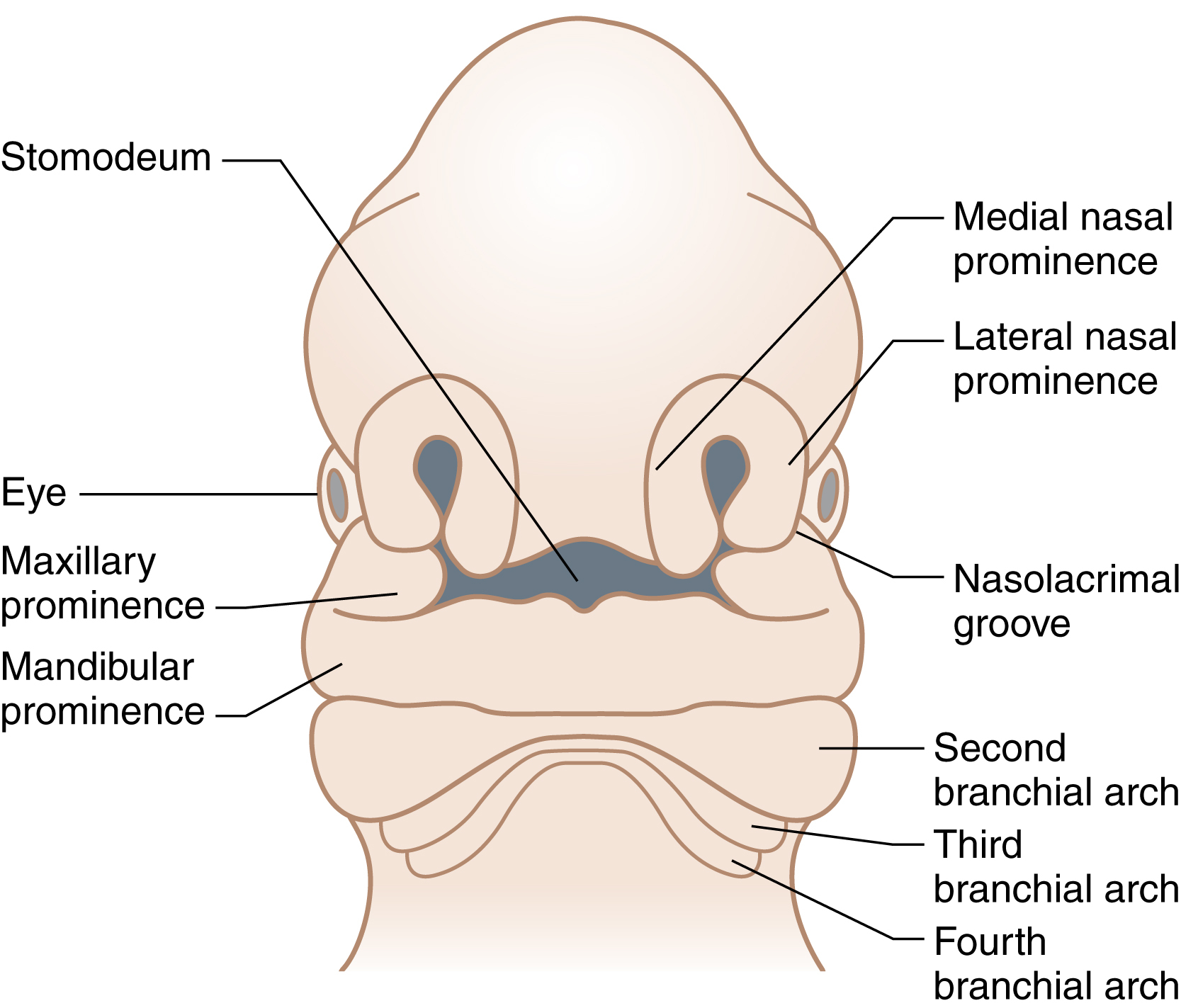
Between the 4th and 7th weeks of gestation, the two medial nasal prominences of the frontonasal process fuse to form the intermaxillary segment ( Fig. 16.1 ), consisting of premaxilla and prolabium. In addition, the two maxillary prominences merge, from which the lateral lip and maxillary arch elements arise. By week 7 of gestation, mesenchymal confluence follows apoptosis of the epithelial seams between the medial nasal and maxillary prominences resulting in the formation a complete upper lip. Failure of fusion of the medial nasal prominence with the ipsilateral maxillary prominence results in a unilateral cleft lip and, if replicated bilaterally, a bilateral cleft lip results. The ratio of unilateral left, unilateral right, and bilateral cleft lip deformity is 6:3:1, respectively. The lateral nasal prominences form the alae of the nose and do not contribute to the upper lip. At the molecular level, several major signaling pathways, including Bmp , Fgf , Shh , and Wnt , are critical for midfacial morphogenesis, and subtle abnormalities in any one of these processes may lead to orofacial clefting.
Cleft lip is defined as a congenital abnormality of the primary palate. It may be complete or incomplete, unilateral or bilateral, and may be associated with a palatal cleft. The forme fruste cleft is qualified by a notch in the vermilion, a visible furrow extending from the edge of the lip to mid-nostril floor and subtle irregularity of the alae. A Simonart band occurs in approximately 30% of patients with a unilateral cleft lip and palate, and describes the small soft tissue bridge, most often devoid of orbicularis oris muscle, that spans the lateral and medial elements of a cleft lip. The integrity of the underlying alveolus is probably of greater clinical relevance than the magnitude of the soft tissue band, although the band will typically diminish the associated nasal deformity.
In the context of sporadic clefting, the risk of unaffected parents with one child with a cleft lip ± palate having a second affected child is approximately 4%, while with two affected children, the risk increases to 9%. If one parent has a cleft lip ± palate, the risk of having an affected child is similarly around 4%, which increases to 17% for a second affected child. The anatomical severity of the cleft has a direct influence on the recurrence risk in first-degree relatives, with the type of cleft being predictive of the nature of the recurrence.
Most obstetric units in the developed world now routinely offer a mid-trimester fetal anomaly ultrasound scan, with facial examination being advocated since 1984. Using 2D antenatal ultrasound, a Norwegian study detected up to 57% of cases of cleft lip ± palate, of which 43% had an associated anomaly; no cases of isolated cleft palate were diagnosed antenatally. Diagnostic accuracy has improved with the advent of 3D sonography, which has led to a sensitivity of 95% and a specificity of 92.3%. In high-risk populations (i.e., those with a positive family history of orofacial clefting), detection rates of 100% have been achieved. Antenatal magnetic resonance imaging offers no particular advantage over ultrasound for the diagnosis of cleft lip, but has significant potential in improving the diagnosis of cleft palate.
Clinical Anatomy
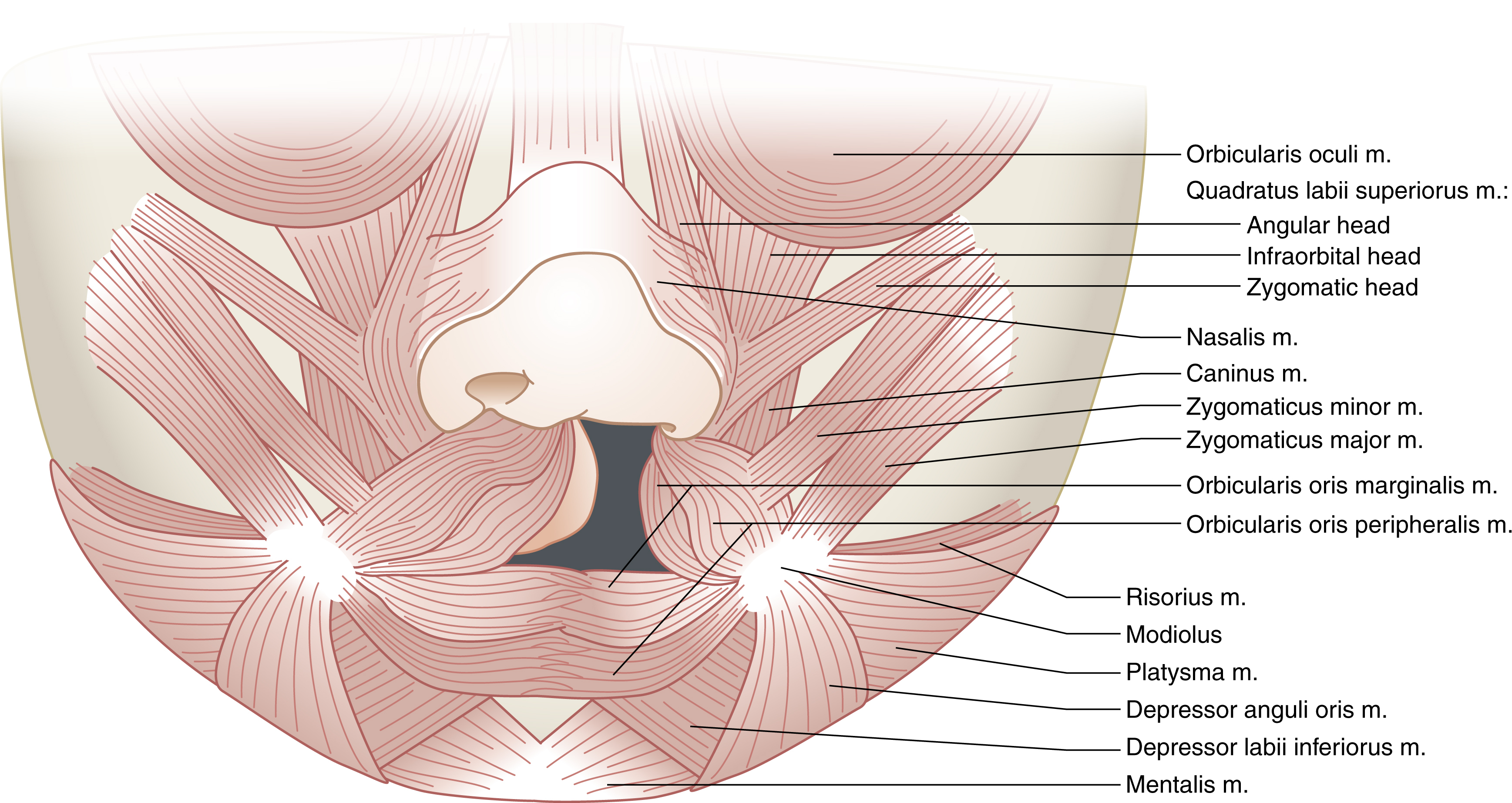
The orbicularis oris is the highly complex sphincteric muscle of the lip that facilitates feeding, speech, and oral continence. It consists of four substantially independent quadrants – upper, lower, left, and right – each of which contains a smaller pars marginalis and a larger pars peripheralis. The surface marking of the junction between the marginalis and peripheralis fibers is the border between the vermilion and skin. The pars peripheralis fibers fan out obliquely from the modioli to interdigitate with the other muscles of facial expression (including zygomaticus major superiorly and depressor anguli oris inferiorly) and terminate within the dermis. Their role is primarily one of articulation and facial expression.
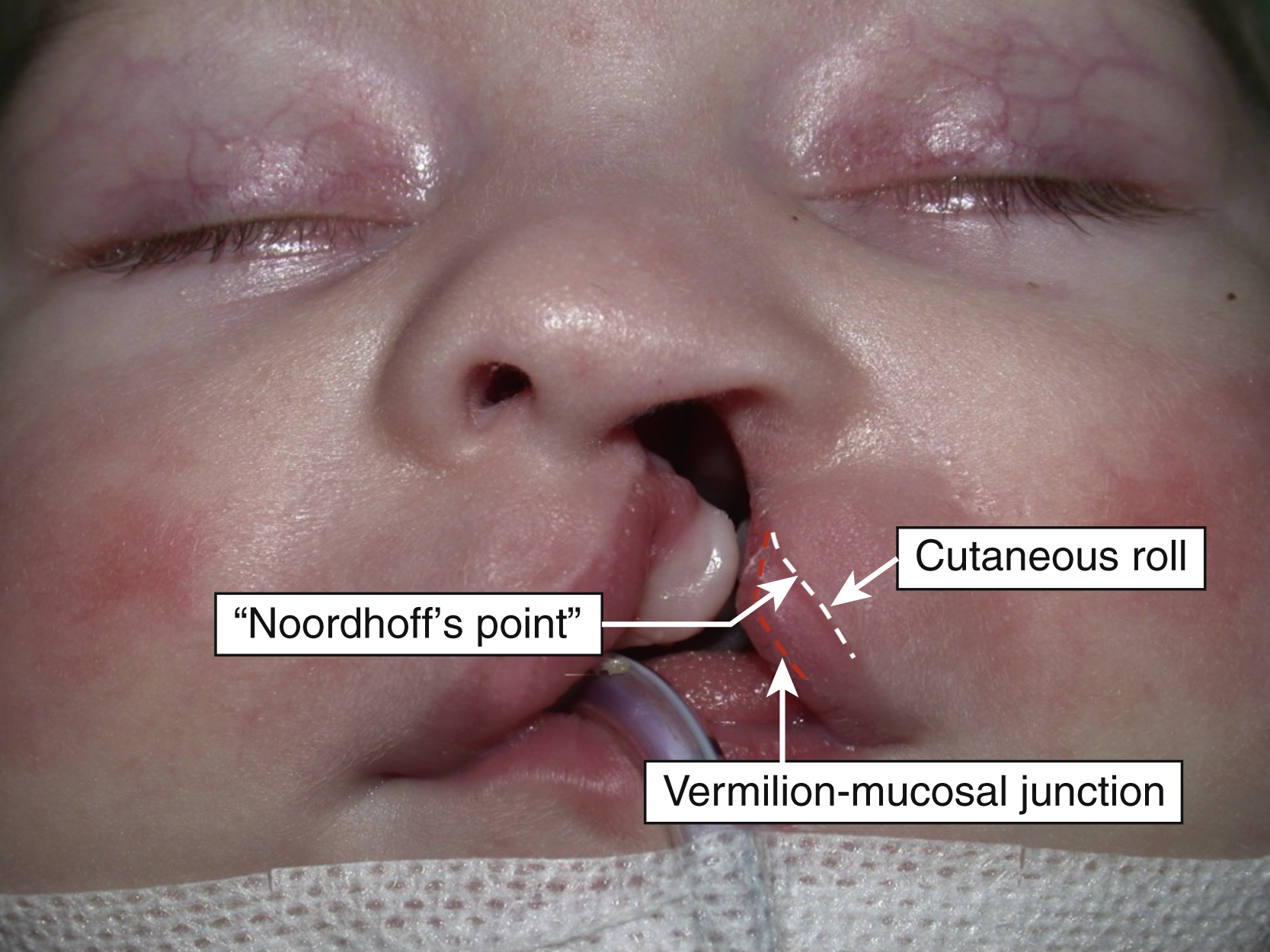
The midline philtral dimple of the non-cleft upper lip is flanked by symmetrical philtral columns that arise from each peak of the Cupid’s bow and curve gently cephalad to the base of the columella. The ridges of the philtral column are created by dermal insertions of the pars peripheralis fibers as they interdigitate in the midline, each crossing approximately 5 mm into the contralateral half of the upper lip. The Cupid’s bow peaks are created by the pull of the levator labii superioris fibers inserting into the base of the ipsilateral philtral column. The cutaneous roll (alternatively, the “white roll” of Gillies or the “white skin roll” of Millard) is the mucocutaneous junction between the vermilion and skin. The cutaneous roll runs from commissure to commissure, but is most prominent centrally at the Cupid’s bow and gradually attenuates laterally. It contains four to five rows of progressively superficially positioned pilosebaceous units containing tiny unpigmented silky vellus hairs, which by reflecting ambient light highlight the contour of the Cupid’s bow. The vermilion has an associated midline tubercle caused by the eversion of opposing pars marginalis fibers. The vermilion–mucosal junction (“red line” of Noordhoff) represents an abrupt transition between the keratinized vermilion and thick nonkeratinized squamous epithelium of the oral mucosa.
In the unilateral cleft lip, the Cupid’s bow is preserved in the medial lip element. The lip height, as measured from the cleft side peak of Cupid’s bow to the base of the columella, is characteristically deficient and the bow is sloped. The cutaneous roll of the entire length of the bow is well preserved. However, there is vermilion height deficiency below the cleft side half of Cupid’s bow. The proposed peak of Cupid’s bow on the lateral lip element has traditionally been less well defined. Noordhoff advocated preserving the proposed base of the philtral column as it is an anatomically determined landmark. He defined it as being located at the point where the cutaneous roll and the vermilion–mucosal junction begin to converge medially ( Fig. 16.2 ). At “Noordhoff’s point”, there is adequate vermilion height (usually matching the height of the vermilion below the non-cleft side peak of Cupid’s bow) and good quality cutaneous roll. Medial to Noordhoff’s point, the quality of these features diminishes.
The height of the lateral lip element (as measured from the subalare to Noordhoff’s point) is frequently different from the height of the non-cleft side (subalare to Cupid’s bow peak). The latter is often excessive in incomplete clefts and usually shorter in complete clefts. The transverse length of the lateral lip element (Noordhoff’s point to the commissure) is almost always shorter than that of the non-cleft side (Cupid’s bow peak to the commissure). Lateral lip element hypoplasia, defined as combined height and transverse length deficiency, is present in almost two thirds of patients with a unilateral cleft.
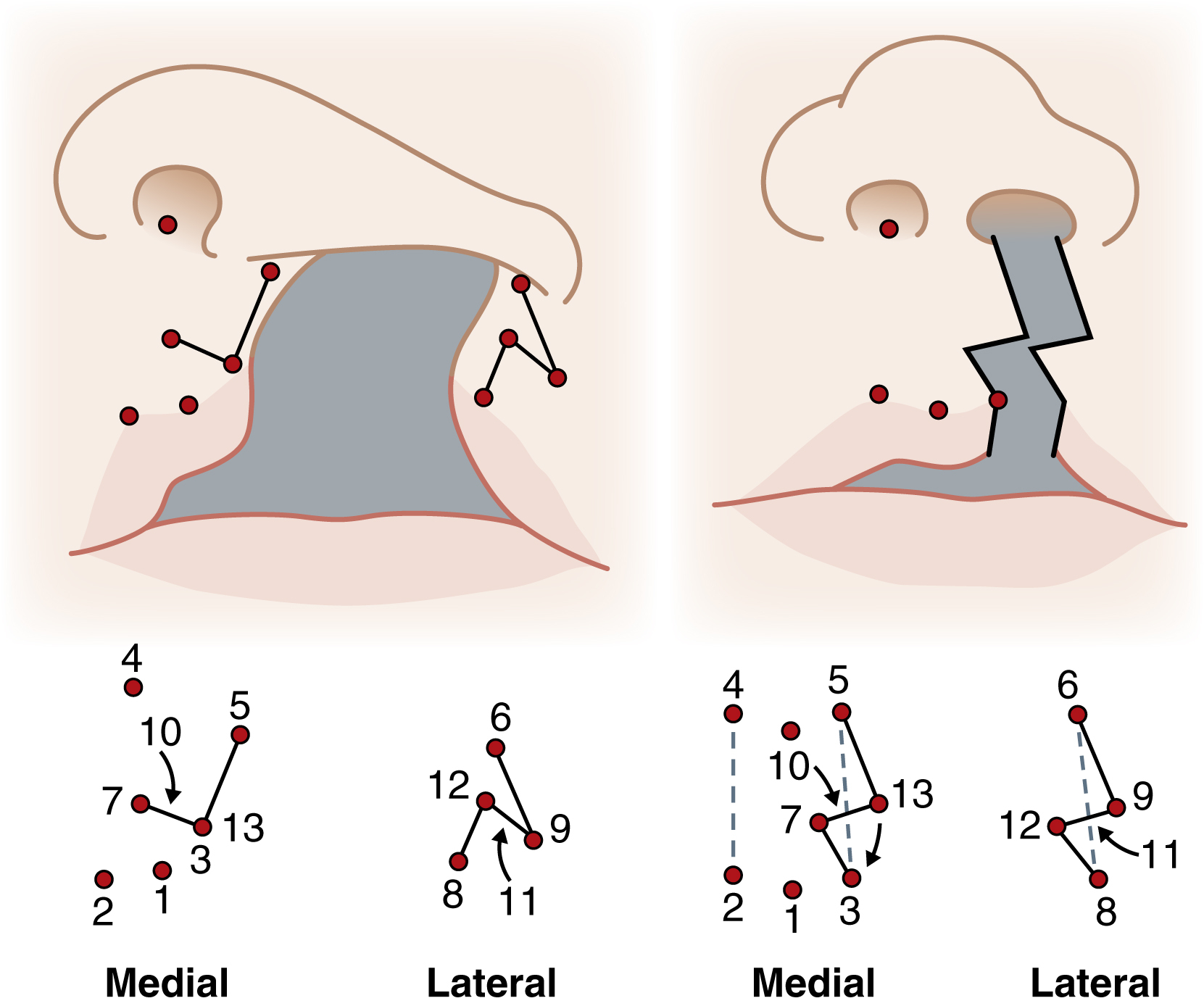
The orbicularis oris muscle is misdirected by the cleft ( Fig. 16.3 ). On the cleft side, the pars superficialis changes direction as it approaches the cleft to run almost vertically to find insertion to the cleft side nostril and periosteum of the piriform aperture. The pars peripheralis inserts into the lateral aspect of the alar and the nasolabial fold; contraction of the lateral lip element orbicularis produces a noticeable bulge in the lateral lip. On the non-cleft side, the orbicularis fibers insert into the base of the columella and nasal septum. Activation of orbicularis exacerbates the nasal deformity by splaying the alar cartilages, broadening the nasal tip, shortening the columella, and deviating the nasal septum to the non-cleft side. Successful correction of the unilateral lip deformity must address these aberrant muscular attachments.
In complete bilateral cleft lip and cleft palate, the prolabium and premaxilla are entirely separated from the lateral lip and maxillary arch elements. The dimensions of the prolabium will vary considerably between affected individuals, but there are some consistent findings. The cutaneous portion of the philtrum is devoid of the dimple and ridges that, in the non-cleft lip, define the shape and dimensions of the philtrum. The cutaneous roll of the prolabium is typically poorly defined when compared with the lateral lip elements, although it is usually better preserved in an incomplete bilateral cleft lip. The height of the prolabial vermilion is inadequate with the superior labial sulcus being shallow, and in some patients, entirely absent. Orbicularis muscle does not enter the prolabium; it therefore lies passively upon the premaxilla, which is protruded and may, in extreme cases, adopt a horizontal posture. The lateral lip elements in the bilateral cleft are similar to the lateral lip element of a unilateral cleft.
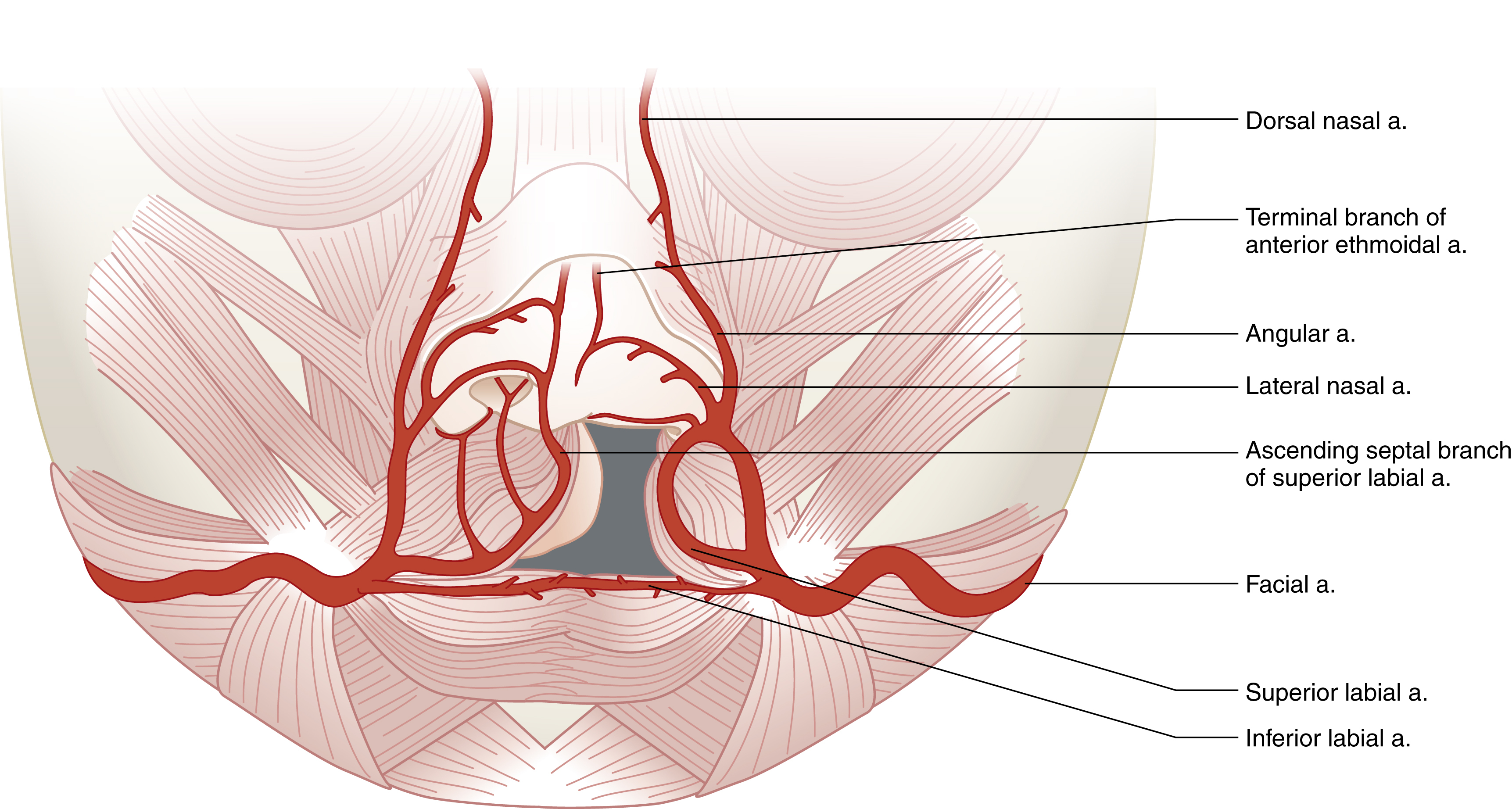
The inferior and superior labial arteries (which arise from the facial artery at the modiolus) are the primary blood supply to the lips ( Fig. 16.4 ). They course close to the free border of the upper and lower lips, lying deep to the orbicularis muscle, juxtaposed to the mucosa, to anastomose with its fellow from the opposite side. The facial artery continues cranially along the line of the nasolabial fold, and after giving off the lateral nasal branch, becomes the angular artery, which then anastomoses with the dorsal nasal artery. The ascending septal branches of the superior labial artery nourish the columella and anastomose with the terminal branches of the anterior ethmoid artery and the lateral nasal artery.
In the unilateral cleft, the superior labial artery on the cleft side is unable to pass horizontally through the lip and therefore anastomoses with the ipsilateral lateral nasal artery. The resultant interruption of the upper lip arterial arcade is of little surgical importance in unilateral cases due to the density of collateral blood supply. However, in complete bilateral clefts, the prolabium receives no input from either the superior labial arteries or, indirectly, via the greater palatine arteries, and is therefore entirely reliant upon the terminal branches of the posterior septal artery (arising from the sphenopalatine artery), the anterior ethmoid artery and the lateral nasal artery.
The characteristics of the nasal deformity in the complete unilateral cleft were first described in 1931, and consists of a depressed cleft side nasal dome and splayed alar cartilages, with eversion of the alar rim and exposure of the nasal lining. The cleft medial and lateral crura are not believed to be hypoplastic based on both cadaveric dissections and intraoperative observations. The cleft alar base is depressed due to the underlying maxillary hypoplasia. Furthermore, anomalous insertion of orbicularis oris into the alar base retracts it both laterally and inferiorly. The nasal spine, caudal nasal septum, and columella, together with the premaxilla, are deviated to the non-cleft side due to the unopposed action of the aberrant insertion of orbicularis oris. Nasal obstruction may result from septal deviation, turbinate hypertrophy, or obstruction of the external nasal valve by nasal webbing. In the bilateral cleft nose, the columella is typically short or nearly absent due to deficient soft tissue and the septum may be excessively broad.
Preoperative Assessment
It is essential to ensure that the infant is optimized prior to surgery; significant comorbidities are common in syndromic children and will inevitably require specialist pediatric input. Early liaison with the cleft anesthesia team is recommended, particularly if there are potential airway concerns. Failure to thrive is seen in approximately 40% of children with a palatal cleft and 9% of those with an isolated cleft lip, thus all cleft patients must be closely monitored preoperatively to ensure that they are gaining weight appropriately. Close cooperation between the family and the cleft unit (via the clinical nurse specialist, dietician, and/or feeding specialist) is essential at this stage.
Although probably less controversial than the timing of palatal closure, currently no global consensus exists for the optimal timing for cheiloplasty. In 1966, Wilhelmsen and Musgrave proposed the “rule of tens” as a criterion for lip surgery: weight greater than 10 pounds (4.5 kg), hemoglobin over 10 g/dL and age over 10 weeks (which replaced a white cell count of less than 10 × 10 3 per mm 3 in their original iteration). Millard observed that lip closure could occur at any time from birth to old age, and he advocated waiting until the child was 3 months of age as this achieved the best results in his opinion. Indeed, the majority of cleft centers defer surgery until the age of 3–6 months, since it allows the optimization of underlying medical issues, minimizes the anesthetic risks, and enables time for presurgical orthopedic treatment if indicated.
Straith performed neonatal lip repair under local anesthesia in the 1940s and many cleft centers continue to perform neonatal cleft lip repair (usually under general anesthetic) sometimes as early as 48 hours of age. It has been argued that with modern specialist neonatal care and anesthetic support, the perioperative risks are minimized, and neonatal repair potentially facilitates improved integration of the child into the family network. There is little evidence to suggest that operating on neonatal cleft lips is unsafe. Although parents may express preference for earlier surgical intervention, there is no evidence of significant psychological morbidity in mothers when delaying repair until the age of 3 months. The concept of an intrauterine cleft lip repair has garnered much interest due to the potential for scarless wound healing prior to 24 weeks’ gestation. Furthermore, fetal repair might reasonably be expected to reduce the magnitude of the secondary “downstream” dentoalveolar and midfacial deformities. However, the technical challenges are vast, and although feasible in both small (murine and lapine) and large (ovine) animal models, albeit with guarded esthetic and functional results, the perceived benefits of fetal repair do not currently outweigh the significant risks of such early intervention.
The role of preoperative microbiological analysis in an attempt to predict the nasal and oropharyngeal flora at the time of cleft surgery is unhelpful, and culture results appear to have no influence on postoperative outcome regardless of whether antibiotics were used. If children with an unrepaired cleft lip and palate undergo preoperative microbiological analysis (with swabs taken from the nasopharynx and oropharynx), approximately 30% will have positive cultures, with the predominant pathogen being Staphylococcus aureus , whilst beta-hemolytic streptococci were isolated in a small proportion of patients. The clinical significance of these results is unclear and debate continues as to whether preoperative microbiology analysis is justified. The evidence for cancelling an elective cleft procedure if a child has a concurrent upper respiratory tract infection remains ambiguous, although most cleft surgeons are cognisant of the increased postoperative risks, and would therefore be reluctant to proceed, favoring an honorable deferral for 4 weeks until the child has fully recovered.
A typical treatment pathway, from antenatal diagnosis to adulthood, for a child with a unilateral complete cleft lip and palate is outlined in Table 16.1 ; comparison is made between The Hospital for Sick Children in Toronto, Canada, and the Spires Cleft Centre in Oxford, UK. Whilst a child with an isolated incomplete cleft lip may require just the single operation, the burden of care in the case of a complete bilateral cleft of the lip and palate is far more substantial.
| Patient Age | Hospital for Sick Children, Toronto | Spires Cleft Centre, Oxford |
|---|---|---|
| Prenatal diagnosis | Genetic counseling (if requested by family) Parental consultation with cleft surgeon | Genetic counseling (if requested by family) Parental consultation with cleft clinical nurse specialist |
| 2 weeks | Presurgical orthopedics (if indicated) | Nil |
| 3–6 months | Cleft lip repair and primary nasal correction | Cleft lip repair, vomerine flap closure of hard palate and primary nasal correction |
| 9–14 months | Complete palate repair ± grommets | Soft palate repair ± grommets |
| ≥3 years as required | Lip revision (if indicated) | Lip revision (if indicated) |
| ≥4 years as required | Speech surgery (if indicated) | Speech surgery (if indicated) |
| ≥7 years as required | Lobule rhinoplasty (if indicated) | Nil |
| 8–10 years (mixed dentition) | Alveolar bone graft from iliac crest | Alveolar bone graft from iliac crest |
| ≥7 years as required | Definitive septorhinoplasty (if indicated) | Nil |
| ≥16–18 years (skeletal maturity) as required | Orthographic surgery (if indicated) | Orthographic surgery and/or Definitive cleft septorhinoplasty (if indicated) |
Presurgical Orthopedics
Historically, the first record of facial binding in order to realign the premaxilla in a complete bilateral cleft was in 1686. In the context of a complete unilateral cleft lip, presurgical orthopedics (PSO) is defined as the use of a device to improve the alignment of the maxillary arch segments in order to facilitate lip repair, and was first reported by McNeil in 1950, by utilizing a removable intraoral plate, and subsequently popularized by Burston. The principles have also been applied to the complete bilateral cleft lip in order to correct the protruded premaxilla.
PSO devices may be passive, such as a dental plate or facial strapping, or active, such as Latham’s appliance, which is pinned to the child’s maxilla, and is adjusted by turning an integral coaxial screw that gradually aligns the alveolar segments. In 1999, Grayson et al introduced the concept of nasoalveolar molding (NAM), whereby the oral plate has nasal prong extensions that reposition the deformed nasal cartilages and lengthen the columella ( Fig. 16.5 ). The resultant approximation of the alveolar segments allows the surgeon to perform a primary gingivoperiosteoplasty at the time of the lip repair, which is said to limit the need for secondary alveolar bone grafting in up to 60% of patients. In those institutions where PSO/NAM is not practiced, alternative strategies can be utilized to reduce alveolar cleft width, such as single-layer vomerine flap closure of the hard palate at the time of lip repair, with subsequent secondary bone grafting of the alveolus.

In spite of considerable enthusiasm for the deployment of PSO/NAM by its proponents, its adoption is by no means universal, with some units reserving its use for more severe deformities such as the wide unilateral cleft or asymmetrical bilateral cleft, while many units do not offer it as a treatment option. This may, in part, reflect concerns regarding the additional burden of care placed on families undergoing PSO/NAM treatment with the associated healthcare costs incurred. Moreover, robust evidence in support of the long-term positive effects of PSO or NAM is lacking; although as any surgeon who has struggled with a difficult primary lip repair may testify, the short-term benefits cannot be completely ignored. A recent systematic review of the literature failed to demonstrate a long-term benefit in the use of PSO. While a systematic review examining the evidence for NAM reported that although there is a trend towards a positive effect, the results are inconsistent regarding long-term changes in nasal symmetry. In 2013 Sommerlad presented the interim results of a randomized controlled study comparing PSO with controls in complete unilateral cleft lip and palate patients; no difference in esthetic or functional outcomes could be discerned at their 5-year and 10-year audit assessments. The issue of PSO/NAM has a tendency to polarize opinion in the worldwide cleft community, a position that is unlikely to change until randomized controlled trial evidence with long-term follow-up becomes available for scrutiny.
Unilateral Cleft Lip Repair
The first recorded cheiloplasty was performed in China in AD 390. In renaissance Europe, Paré was extremely influential, with contemporaneous texts describing the scarification (“paring”) of the cleft margins and approximation of the raw edges using needles and sutures. Husson first recognized that by creating curved incisions, a degree of lengthening of the lip repair could be achieved on wound apposition; a technique later refined by both Rose and Thompson. In 1844 Mirault identified that straight-line scars resulted in unsightly lip shortening, with the potential for notching, and introduced the concept of a triangular flap from the lateral lip element to both lengthen the lip and disrupt the scar. In 1949, LeMesurier recognized the importance of reconstructing the Cupid’s bow using a quadrilateral flap from the lateral lip element, although it was Tennison who preserved the anatomy of the bow, and Randall who reduced the size of the triangular flap. Millard introduced his rotation-advancement technique in 1957, which has subsequently undergone numerous modifications. In 2005 Fisher published his anatomical subunit approximation technique, which utilizes the wound-lengthening principles of Rose and Thompson with the anatomic subunit approach of Berget and Mennick.
Principles of Surgical Repair
Regardless of the surgical technique employed, the principal goals of unilateral cleft lip repair remain constant. These include approximation of the medial and lateral lip elements at all levels (i.e., nostril sill, cutaneous roll, and vermilion–cutaneous junction) without loss of natural landmarks. Balance should be achieved by providing length where tissue is short and excision where height is excessive; poor quality tissue at the cleft margins should ideally be discarded. The scar of union should be placed along natural lines, with appreciation of the anatomical subunits of the nasolabial complex. The nostril margins should be of equal circumference and the alar bases should be symmetric from the anterior view, with careful attention paid to reconstruction of a natural “nostril sill roll.” Complete release of the aberrant attachments of the orbicularis oris muscle must be performed before undertaking a functional muscle reconstruction.
The height of the non-cleft side (i.e., the philtral column length from the lip–columellar crease to the Cupid’s bow peak) provides the dimension that must be created by the cleft side reconstruction. The medial cleft side height (i.e., the philtral column length from the lip–columellar crease to the projected Cupid’s bow peak) is short and will necessitate lengthening from the lateral cleft side lip height. The entire length of the Cupid’s bow should be preserved in the medial lip element. In the lateral lip element, Noordhoff’s point should be conserved and used to form the base of the philtral column incision. The cutaneous roll of the medial and lateral lip elements should be approximated in a side-to-side fashion (creating a “butt joint”). Vermilion height deficiency below the cleft side half of Cupid’s bow should be augmented with attention paid to recreating a level vermilion-mucosal junction.
Operative Technique: Tennison–Randall Inferior Triangle Repair
The inferior triangle repair is a Z-plasty where the middle limb of the Z is shared by the incised medial and lateral cleft margins ( Fig. 16.6 ). Whereas Tennison used a bent wire to stencil equal limbs of the Z-plasty scar, Randall refined the technique using calipers and geometric planning in order to minimize the size of the inferior triangle. The “total lip height” of the non-cleft side is measured from a reference point in the nostril sill to the peak of the ipsilateral Cupid’s bow. The “greater lip height” is measured on the medial cleft side from the proposed medial point of closure at the height of the lip in the nostril sill (symmetric with the reference point in the non-cleft side nostril sill) to the peak of the cleft side Cupid’s bow. The difference between the total lip height and the greater lip height (i.e., the “lesser lip height”) stipulates the base width of the inferior triangle required to level Cupid’s bow.