Circumferential Body Lift
Joseph Michaels
Jennifer Capla
DEFINITION
A lower body lift is a combined procedure consisting of an abdominoplasty, lateral thigh lift, and buttock lift.
Addresses the lower truncal skin redundancy in the massive weight loss patient in a circumferential fashion by removing skin excess from the abdomen, hips, lateral thighs, flanks, and buttocks.
ANATOMY
Excess skin can distort a patient’s anatomy.
Knowledge of the superficial fascial system (SFS) as described by Ted Lockwood is important (FIG 1).1
The SFS has zones of adherence. Posteriorly, this is to the spine; anteriorly, it is to the lower borders of the pelvis.
The bony landmarks of the pelvis are commonly used as reference points, specifically the anterior superior iliac spine (ASIS) and the ischium.
Preservation of the inguinal lymph node basin and knowledge of the course of the lateral femoral cutaneous nerve is important to minimize complications.
Abdomen
The borders are the costal margins and xiphoid superiorly, the pubic symphysis inferiorly, and the ASIS laterally.
Zone 1: midabdomen supplied by the deep epigastric arcade
Zone 2: lower abdomen supplied by the external iliac artery
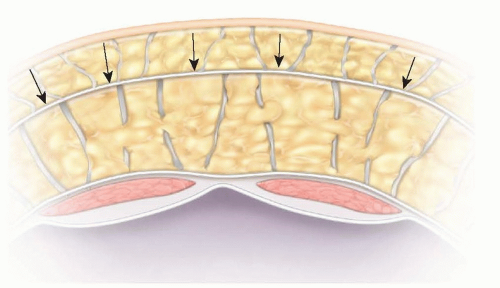
FIG 1 • The superficial fascial system between the superficial and deep fat compartments of the abdomen.
Zone 3: flanks and lateral abdomen supplied by the intercostal, subcostal, and lumbar arteries
Buttocks
Landmarks include the posterior superior iliac spine, the ischial tuberosities inferiorly, and the greater trochanter laterally.
The gluteal fascia will serve as an anchor point for rotational flaps used to preserve and restore buttock volume.
Thighs
This region overlies the greater trochanter and tensor fascia lata. Anteriorly, it extends to the ASIS.
The saddlebag deformity that is commonly seen is a combination of residual adiposity and loose skin.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients generally present with massive weight loss (weight loss greater than 75 lb).
This can lead to various degrees of skin laxity depending on the extent of weight loss, the rate of weight loss, and the patient’s skin elasticity.
Physical examination is focused on the abdomen, lateral thighs, flanks, and buttock.
Patients often present with excess skin in the abdomen and may have an intertriginous rash (erythema intertrigo) in the skinfold. There is also commonly mons ptosis. Excess skin extends to the lateral thigh (saddle bag) region and continues onto the buttock. There is often a sense of deflation in the buttock region.
Abdomen should be evaluated for degree of rectus diastasis, previous incisions, and any associated hernias.
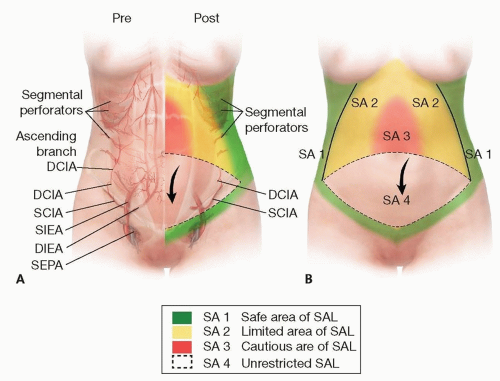 FIG 2 • Blood supply to the abdomen. |
IMAGING
An abdominal CT scan may be helpful if there are any concerns for an abdominal hernia—umbilical, ventral, or incisional. This will allow for better intraoperative planning and the possible need for a general surgeon.
SURGICAL MANAGEMENT
Preoperative Planning
Patients should be at or close to their goal weight and weight stable for a minimum of 3 months.
All massive weight loss patients should undergo a full preoperative evaluation in addition to a nutritional assessment.
Nutritional assessment is an important factor in wound healing and should include albumin, prealbumin, B12, folate, iron, and total iron binding capacity.
Understanding and assessing the patient’s goals is of primary importance.
In front of a mirror, with the patient unclothed, the pinch technique can help provide the patient with a sense of how the tissues will translate and what will be achieved with this procedure. This can also be done with the patient lying down and showing them a picture of the projection (FIG 3).
Determine whether the patient needs added volume in the buttock.
A lower body lift inevitably will flatten the buttock. Gluteal autoaugmentation is considered in patients who desire increased buttock volume and projection.
The markings are the key to the procedure.
Prewarm the operating and all IV fluids to minimize patient hypothermia.
Positioning
The patient is intubated on a stretcher.
The patient is transferred to the operating room table in the prone position with appropriate padding.
Arm boards can be placed on the lower part of the table to widen the bed and to allow for additional abduction of the legs. This will help obtain the maximal lateral thigh lift.
After the lower body lift is performed, the lateral dog-ears are tucked, stapled, and covered with a sterile dressing.
The patient is then repositioned into the supine position for the abdominoplasty portion of the procedure.
Approach
The determination of whether the patient requires additional buttock volume will ultimately determine the approach for the lower body lift.
If none is required, this procedure is simply a circumferential removal of skin, also known as a belt lipectomy.
If increased gluteal projection and volume is necessary, gluteal autoaugmentation or fat transfer will be required.
 FIG 3 • Pinch test to evaluate buttock projection for whether autoaugmentation is needed during a lower body lift.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





