CHAPTER 21 Chemical Peeling: Independent or in Conjunction with Facial Plastic Surgery
The most skilled seamstress can change the dimensions and draping of a piece of cloth but cannot turn a cotton shirt into a silk blouse. Similarly, a surgeon can lift, resect or reposition skin but cannot change the quality, texture, or elasticity of the skin with surgery alone. This reality is a major limitation of surgery.
Fortunately, skin rejuvenation procedures do improve the quality, texture, and elasticity of the skin.1 There are many methods and techniques to rejuvenate the skin including topical cosmeceuticals, dermabrasion, chemical peeling and laser resurfacing. All of these methods are effective in rejuvenating the skin. The most superficial layer, the stratum corneum may be removed with exfoliants, mild alpha hydroxy acids or abrasives. This will give the skin a healthy glow by removing the outer, thickened dead keratin layer and may soften very fine rhytids. Removal of deeper skin layers can be accomplished with dermabrasion, chemical peeling or laser resurfacing. Dermabrasion and chemical peeling are operator dependent for precise control of wound depth. Thus, there is an artistic component to achieving consistent results from these methods. Laser resurfacing, on the other hand, is more precise in regards to wound depth. It is less operator-dependent and theoretically more safe than the other methods. It is extremely important to be well versed in all techniques of skin rejuvenation as well as the basics of wound healing. The authors perform all of the above techniques, individualizing the techniques to the patient’s needs and desires (Fig. 21-1). This chapter will concentrate on chemoexfoliation as the time tested mainstay and still popular method of skin rejuvenation.

Introduction
Chemical peeling or chemoexfoliation, is the process in which the skin is wounded or burned with a chemical agent. The zone of cellular destruction and depth of the wound is dependent on several variables including the peeling agent, the concentration of the agent, skin thickness and skin permeability.1 The immediate reaction of the skin is a second-degree, chemically induced burn. Inflammation begins shortly after the peel and extends variably into the epidermis and dermis. The inflam-matory response peaks at 48 hours but skin rejuvenation and collagen remodeling may last for weeks or months. Regeneration of the surface epithelium begins almost immediately and is usually complete by 5–14 days.
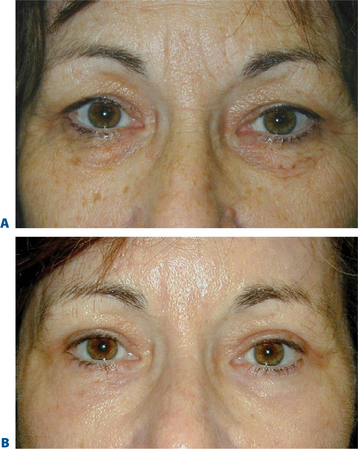
No matter which technique is utilized, if the wounding depth is significant there will be some permanent changes to the skin. The papillary dermal collagen changes from a wavy pattern to straight and parallel beneath the epidermal layer. The dermis shows fibroblastic proliferation and replacement of much of the old deformed elastic fibers with new elastic fibers.2 Depending upon the degree of wounding and chemicals used, there may be fewer melanocytes both in the basal layer as well as in the dermis. This accounts for the lightening in color after peeling. This lightening, again, is a spectral change and may be permanent depending again upon the degree and agent of wounding. With fewer melanocytes the ability to tan is diminished accordingly. In terms of texture, the skin itself becomes smoother and more light reflective (shinier) which is generally a healthy replacement for the previously sun-damaged skin (Fig. 21-1). The potential increased sun sensitivity due to decreased melanocytes makes sun protective measures very important.
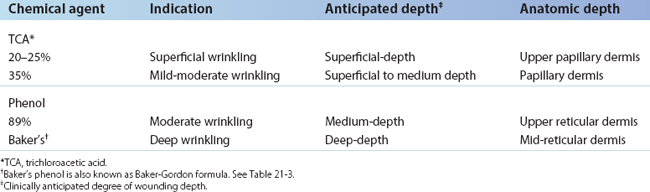
In general, the deeper the wound, the deeper the zone of replacement of old, damaged, and disorganized skin structural elements with new, healthy, and well-organized elements.3 By the same token, the deeper the wound, the greater the potential for scarring and pigment changes. Chemical peels may be divided into three types, graded by the depth of the wound (Table 21-1). Superficial-depth wounding is to the stratum granulosum, papillary dermis. Medium-depth wounding is to the upper reticular dermis. Deep-depth wounding is to the mid-reticular dermis.
Indications and patient selection
Chemical peeling is often performed in conjunction with blepharoplasty, endoscopic brow lifting and facelifting. In general, skin that has been surgically undermined is not peeled at the same time as surgery. If the depth of surgical dissection is subcutaneous, it is possible that superficial damage to the skin from the chemical peel may result in full thickness skin necrosis. However, if the depth of dissection preserves the subdermal vasculature, as in subperiosteal facelifting or transconjunctival blepharoplasty procedures, simultaneous peeling is considered safe.
Simultaneous transconjunctival blepharoplasty and chemical peeling has been performed since 1989.4 The primary aim of lower blepharoplasty is either the removal or repositioning of fat in order to address the undesirable convexity (bulging) of the lower eyelid and/or central midface concavity. Approximately 70 percent of patients who want to undergo lower blepharoplasty have such a small component of excess skin that the risk of the transcutaneous approach outweighs the advantage of removing a few millimeters of vertical skin, particularly when the skin problem is mostly due to actinic damage. The authors have been performing only transconjunctival blepharoplasty approaches on these patients for the past 20 years.
One of the authors (DMM) developed and has refined the technique of simultaneous transconjunctival blepharoplasty and chemical skin peeling since 1989.4 We now all routinely use this combination procedure (Fig. 21-2). The 70 percent of patients in whom skin removal has too great a potential risk will all potentially benefit from simultaneous transconjunctival blepharoplasty and chemical peel rejuvenation of the skin of the lower eyelids; in fact, many of the 30 percent in whom the risk of blepharoplasty is acceptable can also significantly benefit from this simultaneous blepharoplasty and chemical peel without the risk of an infralash incision.
Chemical peeling is also performed in conjunction with facelifting procedures. In general, lower facelifting procedures will improve the jowls and tighten the neck. It does little to improve the perioral rhytids, general loss of skin elasticity and dyschromia. Upper facelifting procedures (forehead lifts) will elevate the brows and reduce dynamic wrinkles. It will, however, not delete the permanent creases that are often found in the glabella and forehead regions. Depending on the degree and depth of these wrinkles, a variety of chemical peels can safely be performed simultaneously in areas that have not been surgically undermined. Thus, it is common for us to simultaneously perform an upper and lower facelift, transconjunctival blepharoplasty along with perioral, forehead and lower eyelid chemical peeling.
Evaluating the skin5
Hypopigmentation after chemical peel is a concern. Certainly, the issue of skin color change must be thoroughly discussed with the patient preoperatively. The deeper the wounding the more potential for hypopigmentation. In addition, as a chemical, phenol is melanotoxic. Originally it was thought that permanent hypopigmentation presented little or no problem for light-skinned patients (Fitzpatrick’s classifications I–II6) (Table 21-2). We have come to realize that these very light skinned patients will have significant whitening of their skin, especially after deep peels. If a full-faced peel is performed and the edges of the peeling are feathered onto the neck, the hypopigmentation can be easily camouflaged. If, however, individual regions are only peeled, the color contrast between the peeled and non-peeled zones can be quite noticeable. This will force the patient to require a base or foundation make-up to blend the peeled and non-peeled regions.
Table 21-2 Reaction to sun by skin pigment type
| Classification (Fitzpatrick)6 | Pigment type | Reaction to sun |
|---|---|---|
| I | Minimum pigment | Always burns, never tans |
| II | Blue eyes, red hair | Usually burns, rarely tans |
| III | Average pigment | Sometimes burns, average tans |
| IV | More pigment | Rarely burns, usually tans |
| V | Much pigment | Minimum burns, mostly tans |
| VI | Most pigment | Never burns, always tans |
Chemexfoliation and wounding agents
Chemical peeling is a commonly performed procedure. The depth (and, therefore, effectiveness) varies with the chemical agent used, its concentration, and the conditions under which it is applied. The wide spectrum of agents and formulas for peeling includes retinoic acid (Retin-A), solid carbon dioxide, sulfur solutions, resorcinol, salicylic acid, alpha-hydroxy acids, trichloroacetic acid (TCA), and phenol and phenol formulas. Table 21-1 lists the most common peeling agents, concentrations, and formulations and the depth to which they can wound.
The surgeon must determine the depth to which he or she wishes to wound the skin, since it is wound depth that determines the potential for the final result. Unfortunately, depth is not simplistically determined by chemical formulas and concentrations, as implied in Table 21-1. Other major factors that help determine wound depth are skin type (Fitzpatrick’s skin classifications I–VI), skin condition and thickness, pretreatment with retinoic acid (Retin-A), alpha-hydroxy acids, alpha-keto acids, low dose cis-retinoic acid, epidermabrasive exfoliants, and defatting preparations. These agents alter the permeability of the skin to the wounding agent. Furthermore, the larger the amount of agent applied, the longer and harder the agent is rubbed onto the skin, and the longer the duration of contact between agent and skin, the deeper the wounding caused by the same agent. Finally, applying tape over the agent (occlusion) drives the chemical deeper into the skin.
Each of the several chemical wounding agents (see Table 21-1) may be used in various strengths. The most common agents, in increasing order of strength, are TCA (15, 20, 25, 35%) and phenol 89 percent. Most wounding agents can be driven deeper into the skin, and thus cause a deeper burn, by occlusion (taping or ointments), wetter applications, multiple applications, or vigorous scrubbing of the agent into the skin. Due to the increased risk of scarring due to uneven penetration, the authors do not use taping as a method of penetration enhancement. Thus, we will not discuss taping in this chapter.
It is thought, though still not conclusively proven, that phenol’s ability to wound increases with the dilution. (That is to say, the more dilute the phenol preparation, the greater the penetration.) Phenol preparations such as Baker-Gordon formula (Table 21-3) dilute the phenol and use additional ingredients. Studies have shown that the most toxic phenol preparation is a phenol and water combination of 2 : 1. Thus, any dilution of full-strength phenol preparation, as occurs when tears run onto the eyelid, may increase the depth of penetration.
Table 21-3 Baker-Gordon chemical peel formula
| 3 ml 89% liquid phenol (USP) |
| 2 ml tap water |
| 8 drops liquid soap (Septisol) |
| 3 drops croton oil |
Related posts:
 Upper Blepharoplasty Combined with Levator Aponeurosis Repair
Upper Blepharoplasty Combined with Levator Aponeurosis Repair
 Brow Lift Techniques
Brow Lift Techniques
 Transconjunctival Approach to Resection of Lower Eyelid Herniated Orbital Fat
Transconjunctival Approach to Resection of Lower Eyelid Herniated Orbital Fat
 Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
 Eyelid and Facial Laser Skin Resurfacing
Eyelid and Facial Laser Skin Resurfacing
 Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


