Acknowledgments
The authors would like to thank Associate Professor Michael Leung in the preparation of this chapter.
Introduction
Defects of the cheek pose a challenge for the reconstructive surgeon. It is a mostly flat and relatively featureless terrain whose superficial appearance conceals a complex arrangement of fascia, arteries, and nerves. Its esthetic significance is associated with its contour, the preservation of which should be a priority for the reconstructive surgeon, though a carelessly-placed scar may also be disfiguring. Fortunately, it is also an area where the surgeon has a number of options for reconstructing defects with excellent functional and cosmetic results.
Anatomy
The cheek comprises one of the original esthetic units of the face as described by Gonzalez-Ulloa. It is bordered by the eye, nose, lips, chin, mandible, and ear. Functionally, it is important for mastication, swallowing, and speech. It forms a discrete esthetic unit of the face whose appearance was classically described by Menick as “a relatively flat, expansive surface, except for the soft roundness of the nasolabial folds and the cheek prominences,” that acts as a “picture frame” for the central face. As such, its contour is of utmost importance.
It is bordered by the infraorbital rim and zygomatic arch superiorly, the lower lid-cheek junction, nasofacial junction, nasolabial fold, marionette line, and labiomandibular crease medially, the mandible inferiorly, and the preauricular contours of the tragus and helix of the ear laterally.
Esthetic Subunits
Traditionally, the cheek may be divided into four subunits: medial, lateral, buccal, and zygomatic. , In some texts, infraorbital and parotidomasseteric subunits are described, which are roughly analogous to the medial and lateral subunits, respectively. Taken together, the medial, zygomatic, and buccal subunits constitute the midcheek.
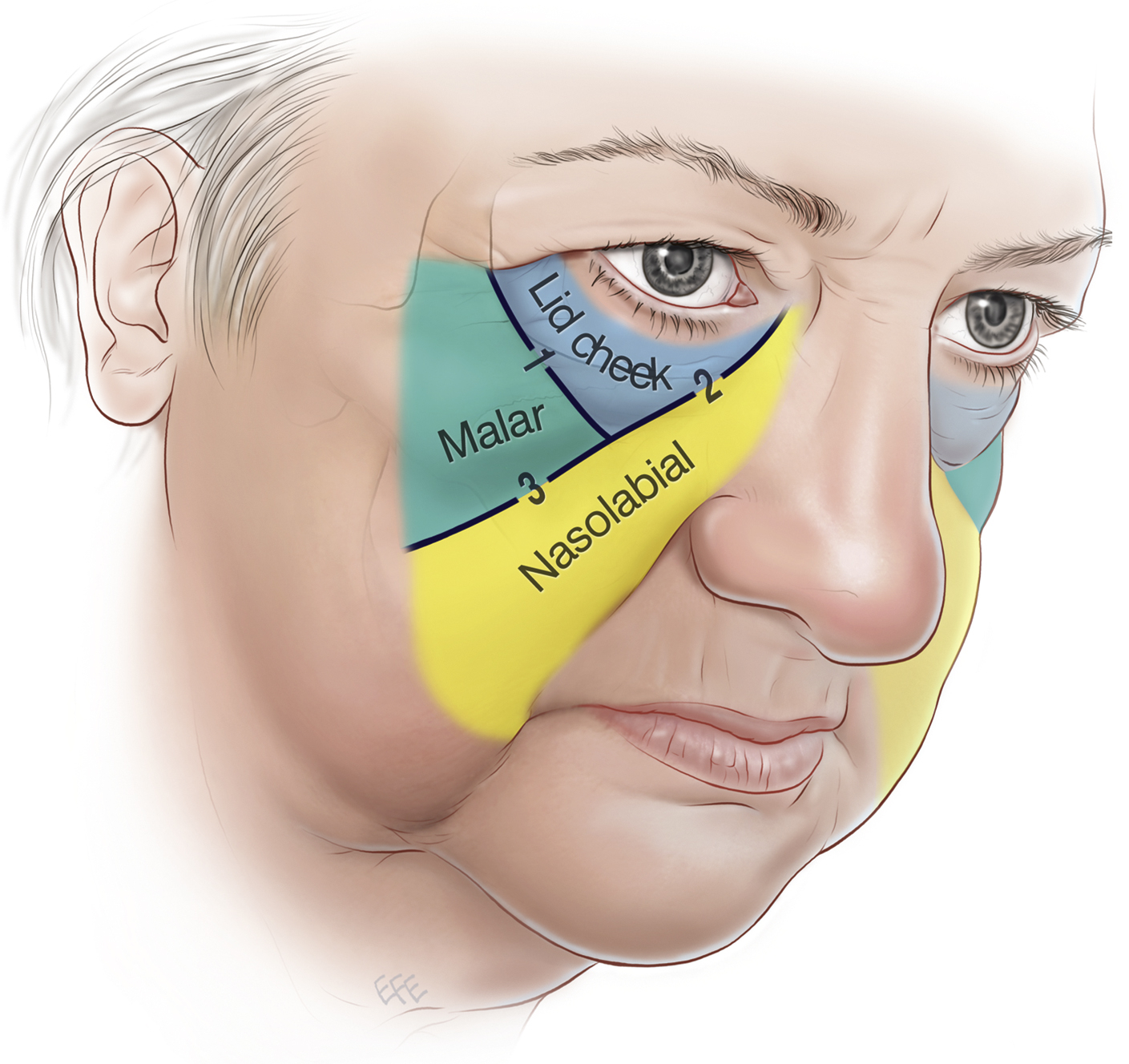
Work by Mendelson has redefined the midcheek by taking into account fascial spaces and retaining ligaments identified in anatomical studies ( Fig. 28.1 ). He divides the midcheek, which is itself defined as the area between the lower eyelid and nasolabial junction, into the lid-cheek, malar, and nasolabial segments, separated by the palpebromalar groove and nasojugal groove. This categorization more faithfully reflects the transition between the thin skin of the eyelid and the distinct contours of the malar and nasolabial segments, particularly in the aging face.
Skeletal
The facial skeleton underlying the cheek consists of zygoma, maxilla, and mandible.
Layers
The layers of soft tissue in the cheek correspond to the basic five layers found in the scalp ( Box 28.1 ). From superficial to deep, the layers are skin, followed by a layer of dense subcutaneous fat which is separated into lobules enclosed by fibrous septa. The third layer, the superficial musculoaponeurotic system, or SMAS, was first described in 1976 by Mitz and Peyronie. The SMAS is continuous with frontalis superiorly and platysma inferiorly, between which it envelops the muscles of facial expression. There is another, looser layer of fat between this and the fifth layer, that of the periosteum or deep fascia, which is often absent in the face where the tissues do not overlie bone or skeletal muscle. In areas of the face not overlying bone, different layers are encountered. For example, in the parotid region this is represented by the parotid fascia, and in the buccal subunit of the cheek, the innermost layer is the buccal mucosa.
- 1.
Dermis
- 2.
Subcutaneous layer
- 3.
Superficial musculoaponeurotic system (SMAS) layer
- 4.
Loose areolar tissue
- 5.
Periosteum and deep fascia, or buccal mucosa
Fascia
Fascial structures provide an anchor between bone and skin and provide soft tissue contours throughout the body. Though there is no deep fascia in the face, the principle remains valid, with fascial condensations fixing the soft tissue of the face to the underlying facial skeleton. The retaining ligaments of the face were first examined by Furnas in 1989. He described several groups of ligaments, that remain essential to our understanding of the soft tissue structure of the cheek, contributing to the formation of the contour of the face ( Box 28.2 ). They have since been studied in some detail and are of particular relevance for esthetic plastic surgical procedures such as rhytidectomy. In reconstruction, it may be necessary to disrupt intact retaining ligaments in order to gain sufficient mobilization of flaps, or to recreate the effect of the retaining ligaments using deep sutures. They are discussed in greater detail in other chapters.
- •
Tear trough ligament
- •
Orbicularis retaining ligament
- •
Zygomatic cutaneous ligaments (McGregor’s patch)
- •
Masseteric cutaneous ligaments
- •
Mandibular cutaneous ligament
- •
Platysma auricular ligament
Muscles
The majority of the muscles of the cheek are muscles of facial expression ( Box 28.3 ). They are embryologically derived from the second branchial arch and are supplied by the nerve of that arch: the facial nerve. The exception is masseter. As a muscle of mastication it is derived from the first branchial arch, and is supplied by the mandibular division of the trigeminal nerve. ,
- •
Orbicularis oculi
- •
Levator labii superioris
- •
Levator labii superioris alaeque nasi
- •
Depressor anguli oris
- •
Risorius
- •
Zygomaticus major
- •
Zygomaticus minor
- •
Platysma
- •
Levator anguli oris
- •
Buccinator
- •
Masseter
Arteries
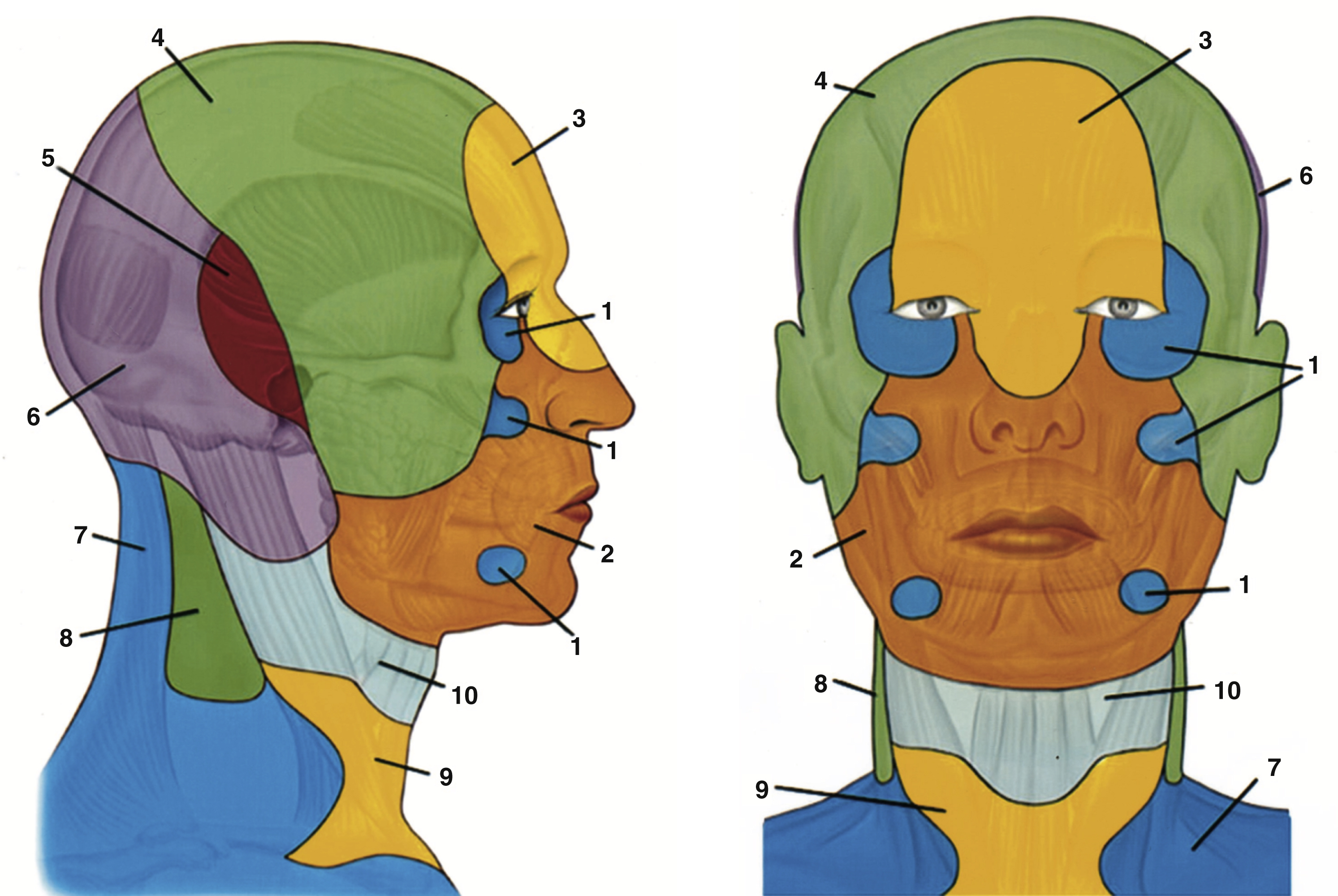
Branches of the external carotid artery supply all the tissues of the cheek. The facial artery (once known as the external maxillary) arises from the external carotid artery in the region of the carotid triangle, crosses the margin of the mandible anterior to the insertion of masseter where it may be palpated, then runs convex anteriorly across the cheek deep to the zygomaticus muscles and becomes the angular artery at the medial canthus. Its named branches are the ascending palatine, tonsillar, submental, glandular, inferior labial, superior labial, and lateral nasal. , The angiosome of the facial artery includes the majority of the cheek ( Fig. 28.2 ).
Three branches of the maxillary artery supply areas on the cheek, one from each of its parts. The inferior alveolar artery branches from the first part of the maxillary artery in the infratemporal fossa, running along the medial surface of the ramus of the mandible to the mandibular foramen. It emerges via the mental foramen and supplies the skin of the chin and inferomedial cheek. The buccal artery branches from the second part of the maxillary artery, then runs anteriorly on lateral pterygoid to supply buccinator and a small area of skin on the medial cheek. The infraorbital artery branches from the third and final part of the maxillary artery in the pterygopalatine fossa, then runs through the infraorbital canal to emerge on the face from the infraorbital foramen. There are extensive anastomoses between all three and branches of the facial artery.
The superficial temporal artery runs upward within the substance of the parotid gland between the TMJ and the external acoustic meatus over the posterior zygomatic arch. It gives off two branches in the cheek: the transverse facial artery, and the zygomatico-orbital artery. The parotid duct of Stensen and the buccal branches of the facial nerve accompany the transverse facial artery, which supplies the skin overlying the parotid gland and lateral cheek. The zygomatico-orbital artery runs superior to the zygomatic arch in parallel with the transverse facial artery as far as the orbicularis oculi muscle.
Veins
The facial vein accompanies the facial artery, running immediately lateral to it, but follows a less tortuous course. The infraorbital vein accompanies the artery in its course and is a tributary of the facial vein. The retromandibular vein is formed by the union of the superficial temporal and maxillary veins from the pterygoid plexus and may be found accompanying the superficial temporal artery. It divides into anterior and posterior branches, the former joining the facial vein before emptying into the internal jugular vein, the latter forming the external jugular vein with the posterior auricular vein.
Lymphatics
The pattern of lymphatic drainage of the cheek roughly mirrors the venous system, and is chiefly to the submental, submandibular, and periauricular nodes. ,
Nerves
The anatomic structure of chief importance in the cheek is the facial nerve. As the sole motor supply to the muscles of facial expression, any facial nerve injury can have significant and lasting effects on patients’ quality of life. After emerging from the stylomastoid foramen the facial nerve enters the parotid gland. From this point on the ramification pattern of the facial nerve is highly variable. In general, upon emerging from the parotid it has frontal, temporal, buccal, mandibular, and cervical branches, and various landmarks have been described for locating individual branches. Depth of facial nerve branches also varies according to the area of the cheek being examined and the presence of tissue spaces, though in general they are deep to the SMAS laterally before becoming more superficial to supply muscles of facial expression medially.
The skin of the cheek, and of the face in general, is supplied almost exclusively by branches of the Vth cranial nerve: the trigeminal. The sole exception is an area of skin overlying the parotid gland and the angle of the mandible, which is supplied by the great auricular nerve, a branch of the cervical plexus. The remainder of the cheek is supplied by branches of the lower two divisions of the trigeminal nerve. The maxillary division provides two branches to the skin of the cheek. The infraorbital nerve supplies the cheek immediately beneath the eyelid, while the zygomaticofacial nerve supplies an area over the zygoma just lateral to the eye. The infraorbital nerve may be blocked by infiltration of local anesthetic around where it exits the infraorbital foramen, which is located below the medial third of the infraorbital margin. The mandibular division also provides two branches. The buccal nerve supplies an area beneath the zygoma, between the distribution of the infraorbital and great auricular nerves. The mental nerve emerges from the mental foramen in line with the second premolar tooth and supplies the lower lip and surrounding skin.
Management
As is the case throughout reconstructive plastic surgery, the approach to reconstructing a cheek defect should be individualized for the patient, considering their overall health, prognosis, and functional status. The defect should be examined and characterized, noting such features as defect site, size, shape, and depth, in addition to wound condition and etiology, and any associated injury, where relevant. Clinical photography may be helpful as a record.
General principles are helpful to bear in mind while planning and executing the reconstruction, and Menick has provided some useful guidelines for reconstruction of facial units, which may be applied to cheek reconstruction. It should be borne in mind that in the cheek the crucial element for a good esthetic result is uniformity of skin color and texture, rather than contour or outline. For this reason, local and regional flaps from adjacent units are generally preferred over grafting. Exceptions to this rule are in cases requiring total facial resurfacing, in which case a complete skin graft or complete flap are preferred to a combination of other techniques.
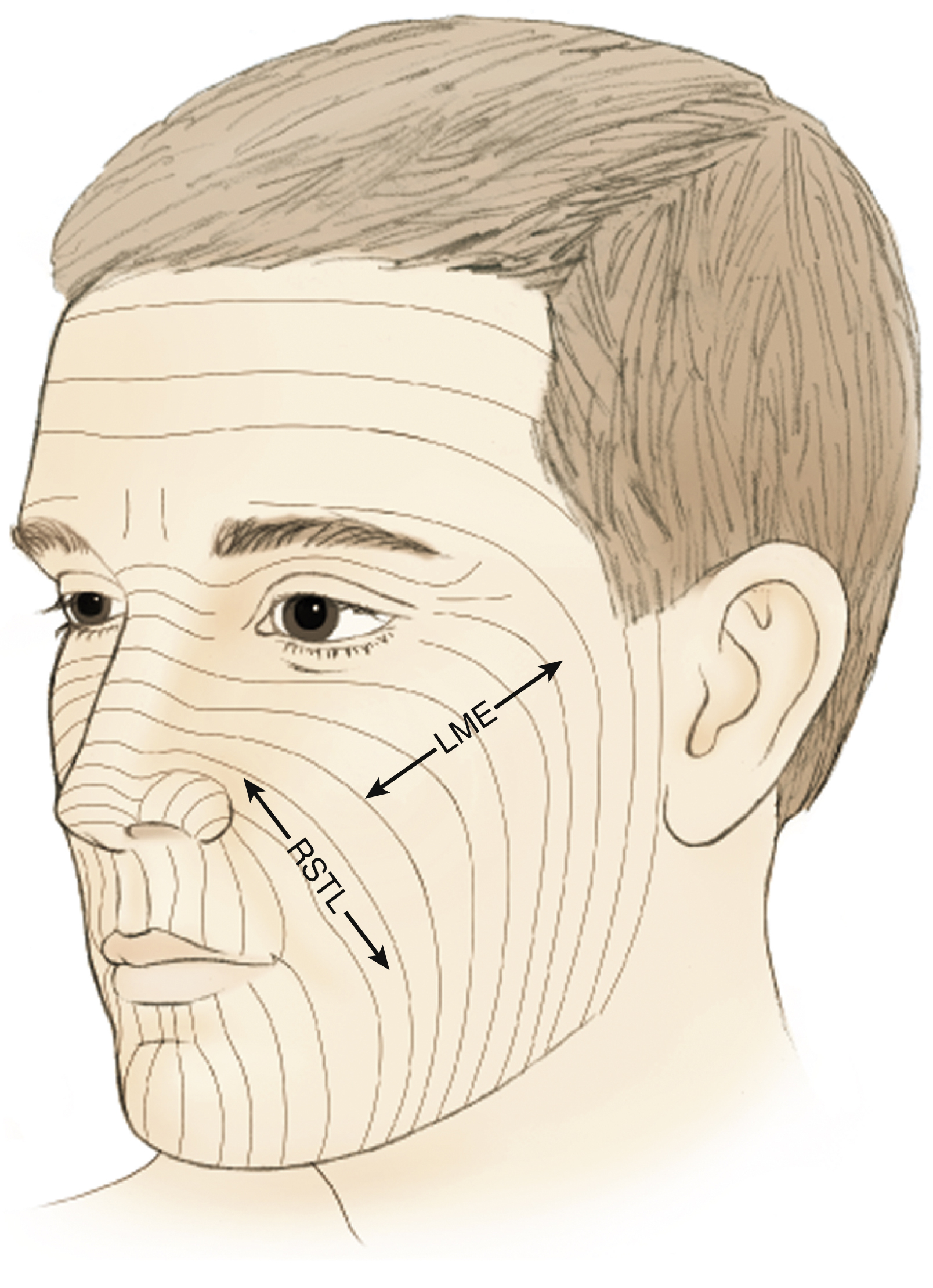
Distant skin is a poor match for facial skin, but for some wounds (large, contaminated, irradiated) transfer of distant tissue using microvascular techniques is the only solution. In these situations a free flap may be used to provide mucosal lining and tissue build, with local and regional flaps mobilized secondarily to provide permanent external skin. For smaller defects which may be amenable to direct closure, scars should be placed either in the borders of esthetic units or in parallel with relaxed skin tension lines (RSTLs), which are perpendicular to lines of maximum skin extensibility ( Fig. 28.3 ).