Abstract
Background: The cheek can be subdivided into seven cheek regions: medial, anterior (maxillary), infraorbital, zygomatic, buccal, mandibular, and preauricular. Cheek reconstruction depends to a great extent upon the wound location in one or more of these seven cheek locations.
Purpose: To provide examples of common repairs done in each cheek region.
Design/Methods: Each cheek region is discussed separately with typical flaps found to be useful in each location.
Results/Outcome: Flaps with and without grafts, if selected carefully for each cheek region, result in an excellent cosmetic outcome that is symmetric with minimal scars.
Summary: Careful selection of the most appropriate skin flap for cheek wound repair results in an excellent functional and cosmetic outcome.
Keywords
flaps by cheek region, complications
As with other facial areas, the goal of cheek reconstruction is to create the “illusion of normality and the perception that all is as it was.” Normality on the cheeks is defined as symmetrical contour, color, and texture. The face is centered by the nose, eyelids, and mouth, and framed by the forehead, chin, and cheeks. Thus reconstruction on the peripheral cheeks will not be as apparent as on the central nose.
Cheek defects are generally repaired by side-to-side closures or flap closures, if possible. Flap closures are used frequently because of the abundant loose cheek tissue, and generally lead to optimal cosmetic results. Grafts and healing by second intention (granulation, contraction, and epidermization) often produce inferior cosmetic results and, except in unusual circumstances that will be discussed later in this chapter, are not commonly used on the cheek.
Like other body areas, cheek reconstruction takes into consideration a number of factors that include the following: location of relaxed skin tension lines (RSTLs); surface anatomy; skin texture; subcutaneous anatomy; patient’s age and medical problems; size, depth, and location of the cheek defect; and previous surgery, radiation, and scars. This chapter will discuss the author’s approach to repair of cheek defects.
Regional Reconstruction Principles
Relaxed Skin Tension Lines
As discussed in Chapters 1 and 2 , the RSTLs generally run inferiorly and posteriorly over the cheek surface. If possible, the long axis of wounds should be directed parallel to these lines, particularly because these wounds will eventuate into scars that run parallel to the wrinkle lines. Also, scars are best placed within the lines and grooves of the cheek borders in the cosmetic unit junctions, such as the preauricular fold, melolabial fold, and nasofacial angle. It should be noted, however, that flap incisions on the cheek rarely spread, even when placed perpendicular to the RSTLs. The reason for this is that in the cheek, although the inherent pull in the direction of the RSTL is more than the pull in the direction perpendicular to the RSTL, it is not very much more.
Surface Anatomy
The cheek boundaries are the preauricular crease, the superior border of the zygomatic arch and malar eminence, the inferior orbital rim, the nasofacial angle, the melolabial crease, and the inferior border of the mandible. The cheek may be roughly divided into seven somewhat overlapping and poorly demarcated subunit areas for the purpose of discussion. These seven areas include the medial, anterior (maxillary), infraorbital, zygomatic, buccal, lateral/preauricular, and mandibular. In each of these areas some flap types are more preferable than others. Many repairs in the cheek cross over and include more than one of these subunits. In some peripheral borders on the cheek, for instance the cheek and eyelid boundary, the border is best not transgressed by a single flap, but rather two flaps, one from the upper eyelid and one from the cheek, so as to reestablish the boundary between the cheek and eyelid zones.
Repairs on the face may be regional (e.g., the whole cheek), as emphasized by Gonzalez-Ulloa, or local (e.g., small flaps on only a portion of the cheek). The subunit principle applied by Burget and Menick to the nose is not as critical on the cheek because the subunits are less distinct. The only defining grooves are at the periphery of the cheek along the cosmetic unit junctions.
The cheek is not a flat surface, but is concave medially, as it extends into the nasofacial sulcus; it is convex over the malar eminence. Only in the lateral cheek and preauricular area is the cheek flat. This uneven topography is important for the surgeon to be mindful of, as cheek reconstruction is three dimensional.
Abundant loose skin exists on the cheeks for flap repairs. This abundant tissue is usually found inferior and lateral to defects to be reconstructed. With age, cheek skin begins to sag, and thus more loose tissue becomes available for repairs. However, in the elderly who have had a facelift procedure or in the young, this normally loose tissue is generally not plentiful. Additionally, if prior surgery has been done on the cheek, the underlying anatomy may have been altered and tissue may not move normally.
Skin Texture
Skin surface characteristics may vary enormously on the cheek from individual to individual and also within the cheek on the same individual. In patients with very oily skin and patulous pores, it may be more difficult to get a good cosmetic result than in patients with smooth nonoily skin. Elderly patients with great skin laxity and a plethora of wrinkles will be easier to reconstruct than the young, who have great elastic skin recoil and no wrinkles. Furthermore, wrinkles afford camouflage for linear, arciform, and flap incision lines. Because of the unique texture of cheek skin, skin grafts in this location generally provide a poor color and texture match. Skin grafts on the cheek appear as patches and should be avoided if possible. The texture of cheek skin may also vary from one cheek region to another. The beard area in a man needs to be kept in mind. The wrong skin in the wrong place may lead to a less than optimal cosmetic result.
Subcutaneous Anatomy
Beneath cheek skin lies an investing fibrous layer, the submuscular aponeurotic system (SMAS). This layer lies between and is attached to the dermis above and the muscles below. Inferiorly SMAS is continuous with the platysma muscle. Deep to the SMAS lies the parotid gland and its duct, facial nerve branches, and superficial muscles of facial expression. All these muscles are supplied by branches of the facial nerve (VII). The buccal branches of the facial nerve over the cheek ramify to such a great extent that any motor loss after reconstruction is usually temporary. The sensory supply to the cheek is mostly from the trigeminal nerve (V). The medial cheek is supplied by the second division (V 2 ) through the infraorbital nerve. The lateral cheek to the mandible is innervated by third division (V 3 ) of the trigeminal nerve. A small lower area of the posterior cheek near the lower ear is supplied by the anterior cutaneous nerve of the neck and by the great auricular nerve, which originates from the cervical plexus (C 2 , C 3 ).
The arteries and veins in the cheek generally need not be taken into account to any great extent when performing superficial cheek flaps. There is such an abundant vascular supply on the head and neck that cheek flaps can be randomly placed in relationship to underlying arteries and nerves. The arterial supply to the cheek is from the external carotid artery, which gives rise to the transverse facial artery and the facial artery. Venous drainage is via the anterior facial vein.
There are, however, two motor nerve branches that are superficial in part of their course on the cheek and that one needs to be wary of. The first is the temporal branch of the facial nerve, which may be superficial as it crosses the zygomatic arch. The second is the marginal mandibular nerve, which crosses over the mandibular artery as it courses along the lower edge of the mandible.
Special Anatomic Structures
There are two special anatomic structures in the cheek worth noting: the buccal fat pad and the parotid duct. The buccal fat pad is a large well-defined area in the central cheek with a large amount of fat. Its importance is that it is a good landmark for Stenson duct, which is the main drainage channel for the parotid gland. The duct courses over the buccal fat pad and descends anterior to it. If Stenson duct is transected and a flap repair done over the leaking area, there will be salivary drainage at the flap edge. Sometimes a Stensen duct partial transection will be difficult to see and is unavoidable. However, should clear fluid drainage occur from the Stensen duct transection, the drainage will generally slow down and go away after a few months. If one sees salivary gland leakage, recanalization of the duct may be attempted with a Silastic tube prior to flap repair; however, in the author’s experience, this procedure is often unsuccessful.
Which Reconstructive Procedure?
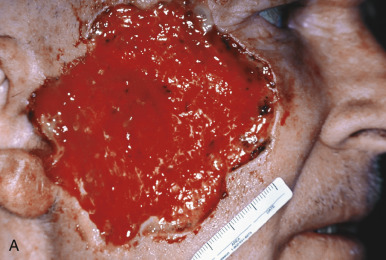
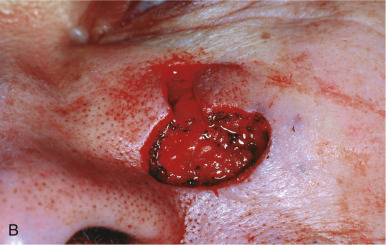
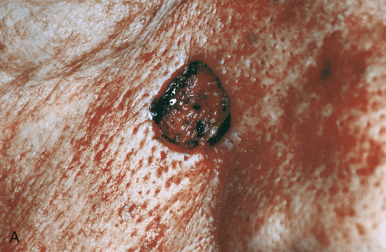
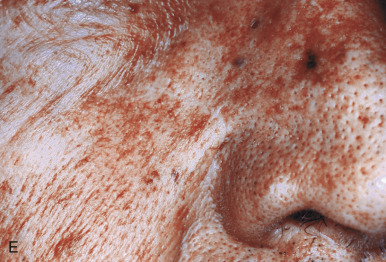
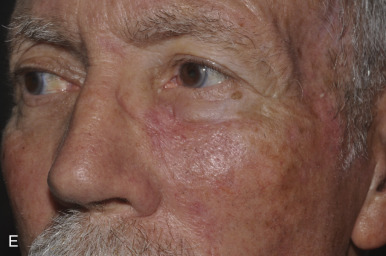
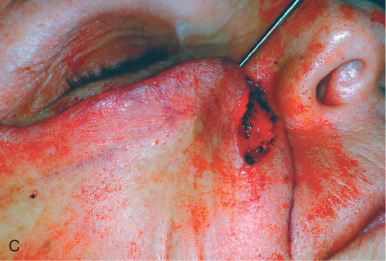
Faced with a cheek defect, how does one select the optimal repair? Generally, healing by second intention on most of the cheek will lead to a noticeable scar, except in the preauricular area. In this latter area, even a very large wound may be allowed to heal by granulation, often resulting in a healed scar with an excellent cosmetic appearance. As mentioned earlier, a skin graft is generally not used on the cheek. A skin graft matches poorly with the surrounding and contralateral cheek skin in color, texture, and degree of hair growth. Furthermore, a skin graft often will not completely fill in a subcutaneous defect, and provides less protection to underlying vessels and nerves than a skin flap. There are, however, two exceptions as to when a skin graft may be useful. The first is to repair a defect that resulted from excision of an aggressive tumor (e.g., angiosarcoma or sebaceous gland carcinoma). In this case, a split-thickness graft can be used immediately to repair the wound defect and prevent contraction. When healed the graft provides a window through which a tumor recurrence could be seen ( Fig. 13.1 ). The second circumstance for placing a split-thickness graft would be to repair a very large defect, which could not be repaired in any other way. Prior to the development of large cheek flaps and cheek–neck rotation flaps, multistaged cheek rotation flaps or large skin grafts were commonly used to repair cheek defects. For a large deep cheek wound with extensive bone exposure, a free flap may be considered. However, a free flap in this area always evenutates into a poor cosmetic result, its thickness will bury tumor, and it requires a prolonged (8–10 hour) operation under general anesthesia. For a very extensive cheek defect that is superficial, a tissue expander could also be considered.


The single largest decision when contemplating a cheek reconstruction is whether to repair a wound with a side-to-side linear closure (complex repair) or a skin flap. The same defect that may be repaired side-to-side in an elderly person with excess skin and wrinkles may require a skin flap for closure in a young person to avoid scar spreading from excess tension.
This author has found empirically that the best way to determine whether a complex repair or a skin flap could be done easily is to lift with skin hooks the ends of the wound up along the RSTLs (see Fig. 13.19B ). If the central wound edges come together easily across the wound with the skin hooks tenting up the wound at the superior and inferior ends, then a side-to-side linear repair may be done. Sometimes, however, a side-to-side repair may be possible, but distortion of the melolabial fold may occur. In this instance, a flap may be preferable. When possible, however, one should close a wound with a side-to-side linear repair, since it will result in fewer incision lines than those from a skin flap.
Reconstruction Philosophy
In reviewing the literature on cheek reconstruction, this author was struck by three trends. The first is that surgeons like to do one specific flap type for one specific defect; the second is that surgeons prefer to close the entire wound at one time. These issues have been raised by other authors. Part of the reason for this approach has been that surgical training programs dogmatically emphasize repairing the whole wound at one time; leaving part of the wound open to heal by granulation is thus unacceptable. The third trend is that even medium-sized wounds on the cheek are repaired by rather large flaps extending into the neck and shoulder, when these same wounds could have been closed with an equally good or better result by smaller, less complicated local flaps. The trend of using cervical neck or cervical pectoral flaps results in excessive surgery. This is not to say there is not a time and place for such flaps, but many of the case examples presented in the literature show medium-sized wounds that could be repaired in other ways.
Flaps to Avoid
On the cheek, two flaps that this author avoids are the subcutaneous island pedicle flap and the bilateral advancement flap. The former usually results in a puffy flap that does not lie flat ; the latter produces too many straight lines that are easily seen. However, some authors continue to recommend these flaps despite showing photographs that demonstrate excessive poorly placed incision lines and a puffy flap.
Flaps by Cheek Region
Medial Cheek
The medial cheek usually has abundant skin laxity. If the wound is small to medium in size and its long axis is oriented obliquely, a side-to-side repair may be done easily ( Fig. 13.2 ). If possible, repairs in this area are closed along or parallel to the nasofacial angle or melolabial fold. Although some authors advise deep “periosteal” tacking sutures for side-to-side linear closures in the nasofacial angle, this author does not do this and feels it is usually unnecessary. For long obliquely oriented wounds on the medial cheek that cannot be closed without excessive tension on the wound edges, the rhombic transposition flap with a double Z-plasty is useful ( Fig. 13.3 ). This flap takes advantage of the inferiolateral loose tissue available on the cheek. The double Z-plasty helps increase the extension of the rhombic flap. The angulated incisions of the rhombic flap and Z-plasties generally blend in well to the surrounding skin over time.









For a medial cheek wound with its long axis oriented horizontally, a side-to-side linear closure obliquely oriented along the RSTLs would lengthen the closure line considerably. Therefore it might be best to consider a flap closure. There are three main flap choices for such a wound in this area: the subcutaneous island pedicle flap, the rhombic transposition flap ( Fig. 13.4 ), and the advancement flap with a back-cut ( Fig. 13.5 ). This author does not like the subcutaneous island pedicle flap for large wounds in this location, as this flap is often puffy, even many months later. When this happens, the puffiness is difficult to correct. Nevertheless, the subcutaneous island pedicle flap may be considered for small wounds just above or within the melolabial fold.








The rhombic transposition flap works well for medium-sized wounds in the medial cheek (see Fig. 13.4 ). As emphasized by Borges, it is important to design the rhombic flap so the base of the flap (i.e., the base of the flap triangle) is perpendicular to the RSTLs on the cheek. Also, as Becker points out, the main rhombic flap tension is at the donor area, and these flaps on the cheek are generally laterally and inferiorly based. Cabrera and Zide further recommend that one base the rhombic flap inferiorly, as this orientation tends to minimize the trapdoor effect due to fluid accumulation, which may or may not be true.
Horizontally oriented defects in the medial cheek are often best repaired with a rotation/advancement flap from the inferior direction (see Fig. 13.5 ). An incision line is made inferiorly along the melolabial crease line, often with a back-cut. The tissue is rotated and advanced superiorly and the back-cut triangle is excised. The incision down the melolabial crease with excision of a Burow triangle rather than a back-cut was described by Imre. I prefer the back-cut triangle because the resultant scar will be well camouflaged by the melolabial crease. Another alternative to the Burow triangle excision is to excise an ellipse at the inferior end of the flap with the lateral side longer than the medial side. On closure the lateral wound edges are displaced superiorly and medially. One problem with the advancement/rotation flap with a back-cut is that medial canthal tenting may occur, particularly when this flap is used to repair horizontally oriented defects high in the medial cheek. To help prevent this problem, Jelks and Jelks advise de-epithelializing the flap tip and fixing it to the medial canthal tendon. The tenting, if bothersome, may be released by a V-to-Y or Z-plasty. For a very large advancement/rotation flap in the medial cheek, one should also place a deep buried “periosteal” suture to hold the downward weight of the flap and decrease wound tension ( Fig. 13.6 ). Another alternative to the inferior cheek advancement flap is the O-to-Z flap. In this case both an inferior and a superior incision are made from opposite sides of the wound. Thus after undermining, advancement and rotation occurs but in opposite directions. To enhance flap movement a back-cut can be made in one or both ends of the O-to-Z flap. As the wound size increases, so does the complexity and difficulty of the flap. For large defects (especially those oriented obliquely) in the medial or anterior cheek area, a whole cheek advancement/rotation flap may be created from the lateral cheek. Using the entire cheek lateral to a large defect as a single flap is considered by some physicians to be ideal because its scar will be less noticeable compared to scars from smaller flaps, which may cross the lines and natural creases of the face. Furthermore, this flap is a very vascular and therefore a safe flap, which rarely has tip necrosis.





The lateral cheek advancement flap has a medial inferior base and a forward and medial destination. The initial incision for a cheek rotation/advancement flap is made horizontally and laterally from the cheek defect extending on top of the orbital rim; as it progresses laterally at the point of the lateral canthus, it is gently curved superiorly above the zygomatic arch to at least the level just above that of the lateral canthus to decrease the chance of ectropion ( Fig. 13.7 ). This latter incision places the vector of any scar contraction in an upward posterior direction so that it will counteract any inferior pull on the lower eyelid. If this flap stops above the zygomatic arch in the temple, it is similar to the Tenzel flap used to close defects on the lower eyelid.





For very large defects of the medial or anterior cheek, the incision should be carried over the zygomatic arch and down the preauricular crease to a point 2 to 3 cm below the earlobe. Here a Burow triangle may be excised and hidden behind the earlobe ( Fig. 13.8 ). The flap is then rotated medially as it is advanced superiorly. It is critical to place tacking sutures along the lateral and inferior lateral orbital rim and the malar eminence to support the heavy flap and prevent ectropion. It is also important to thin the subcutaneous tissue along the superior flap border to match the skin thickness of the lower eyelid.