Chapter 7 Filler Injection of the Eyebrows

Introduction
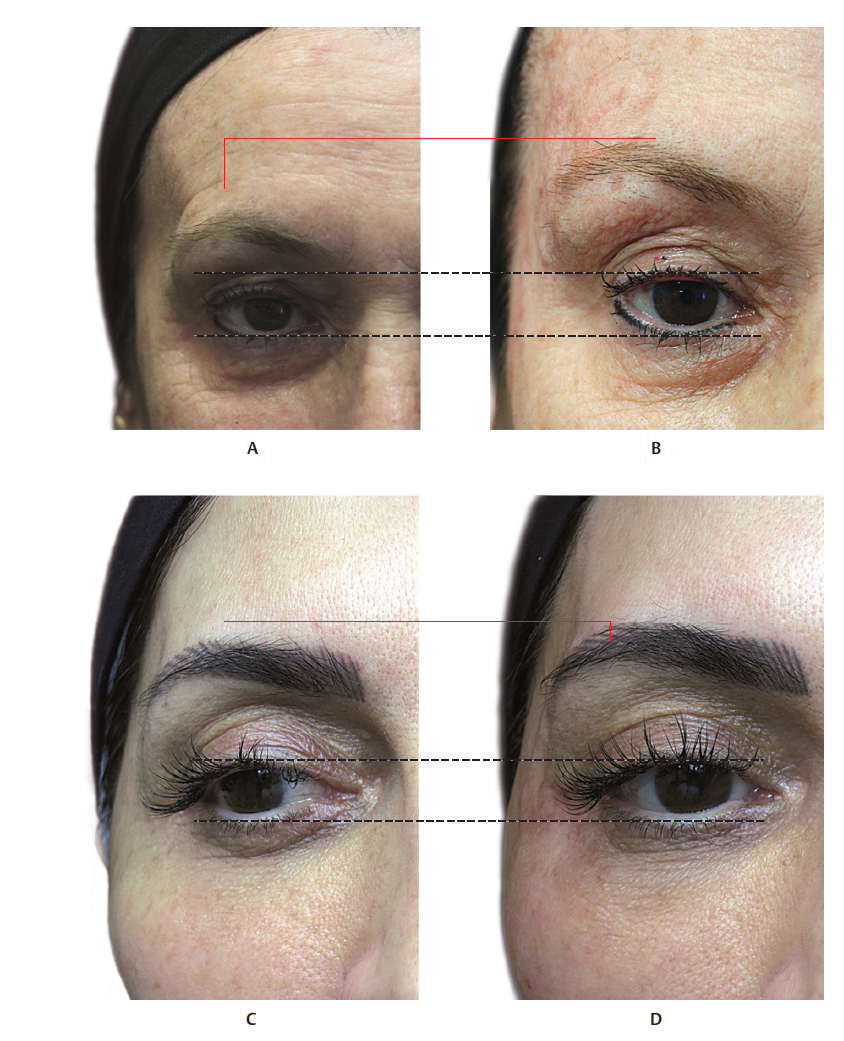
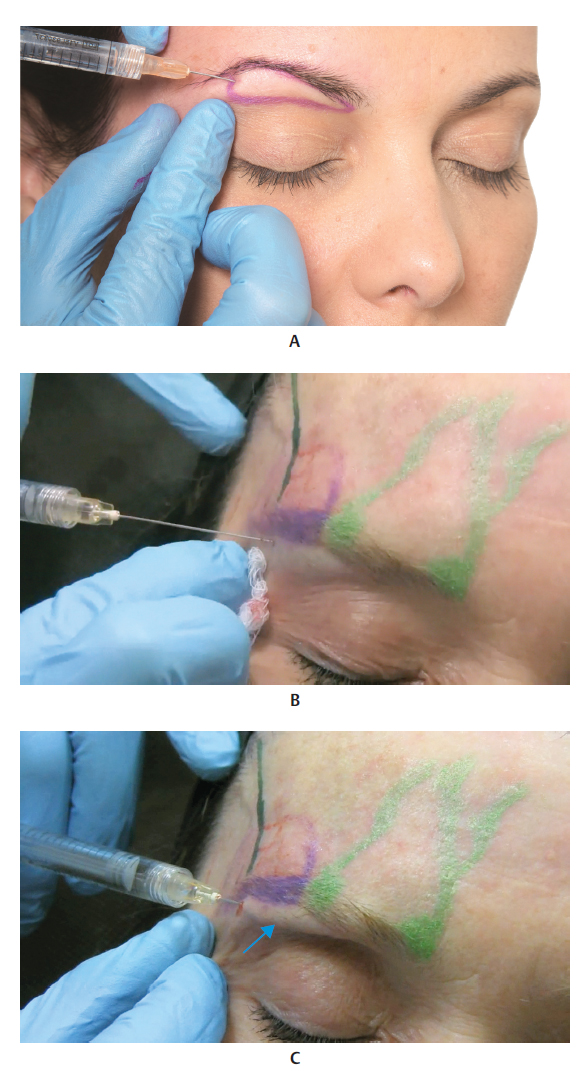
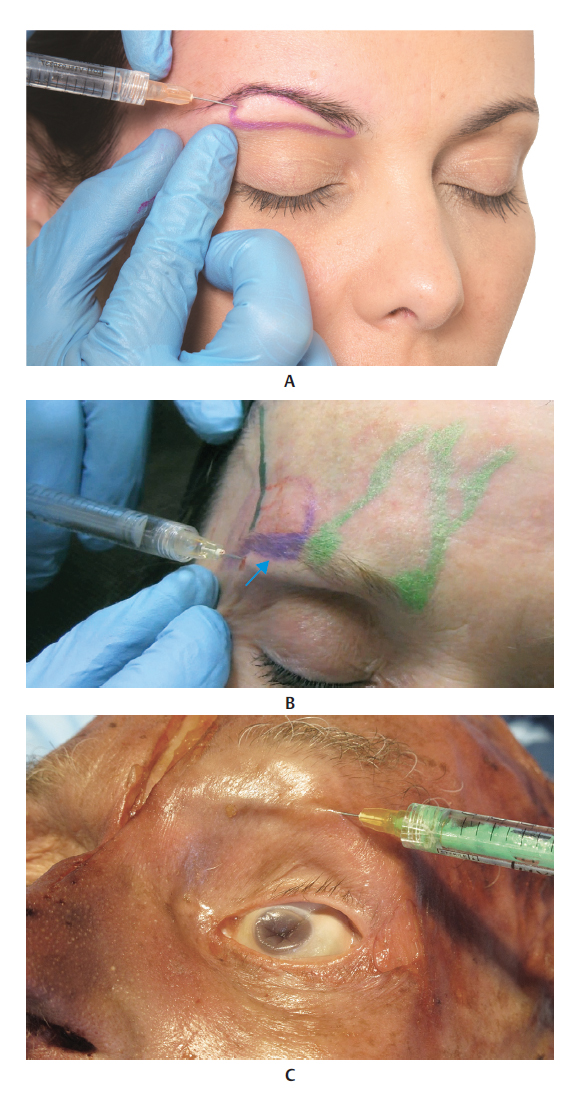
If the eyes are the windows to the soul, then the eyebrows are certainly their frame, as they give the face a format and define the eyes and forehead. The eyebrows are one of the most versatile characteristics of the human face. They influence the perception of beauty, and play a fundamental role in sexual dimorphism, facial recognition, and nonverbal communication, 1 since subtle changes in their position convey different emotions, from anger to surprise. 2 In 1974, Westmore X described the ideal female eyebrow as being slightly curved, with its apex approximately aligned with the lateral corneal limbus. The medial extremity should start at the vertical line of the ala of the nose and the medial palpebral commissure, as shown inFig. 7.1 A. The lateral extremity should end at the oblique lined traced between the lateral ala of the nose and the lateral palpebral commissure. Male eyebrows have a similar medial and lateral alignment but are generally lower and straighter. 2
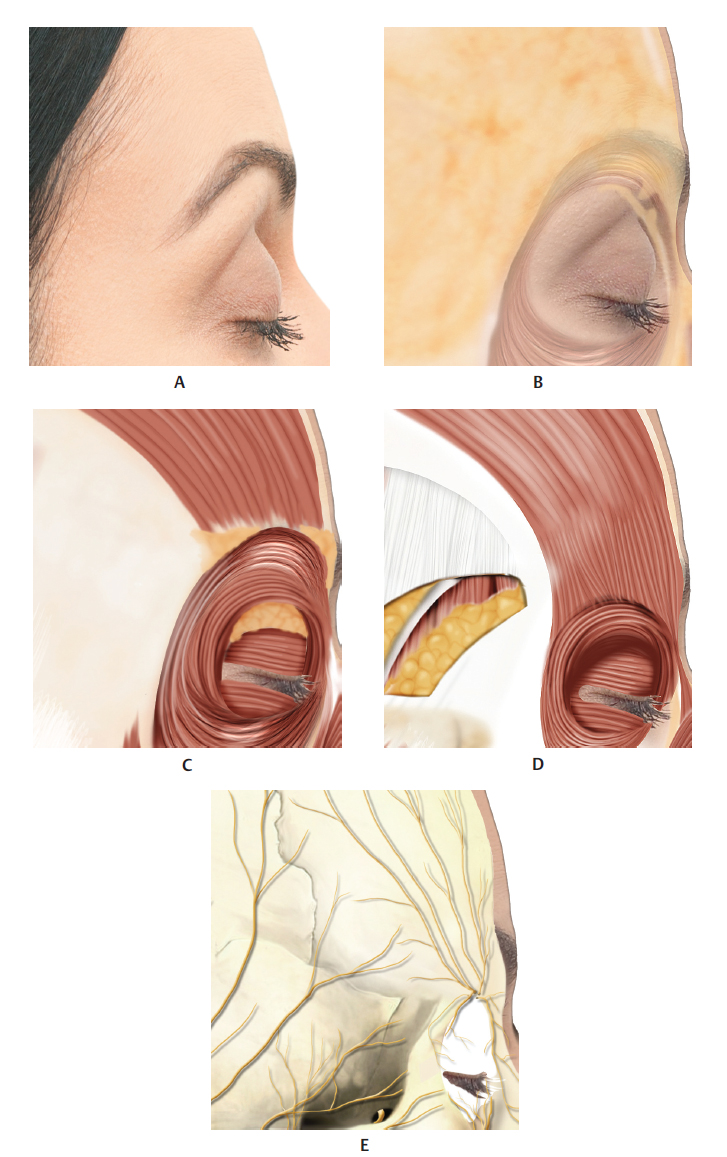
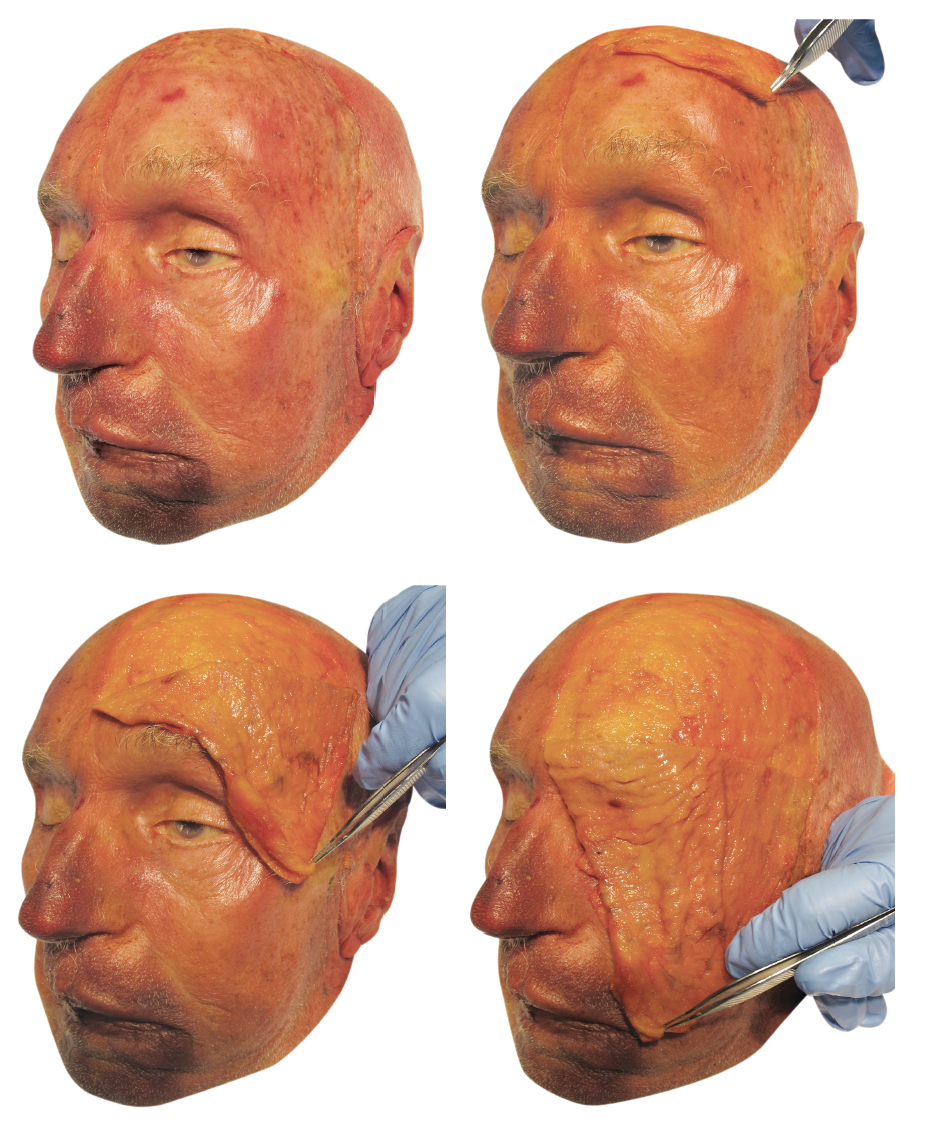
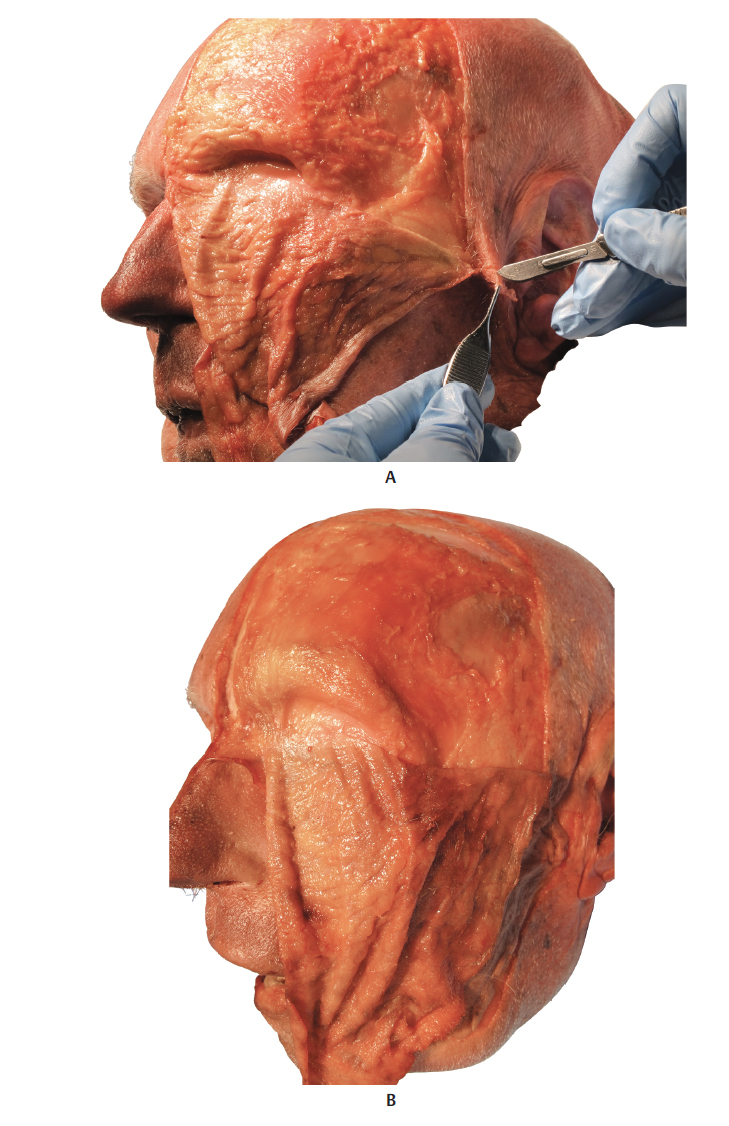
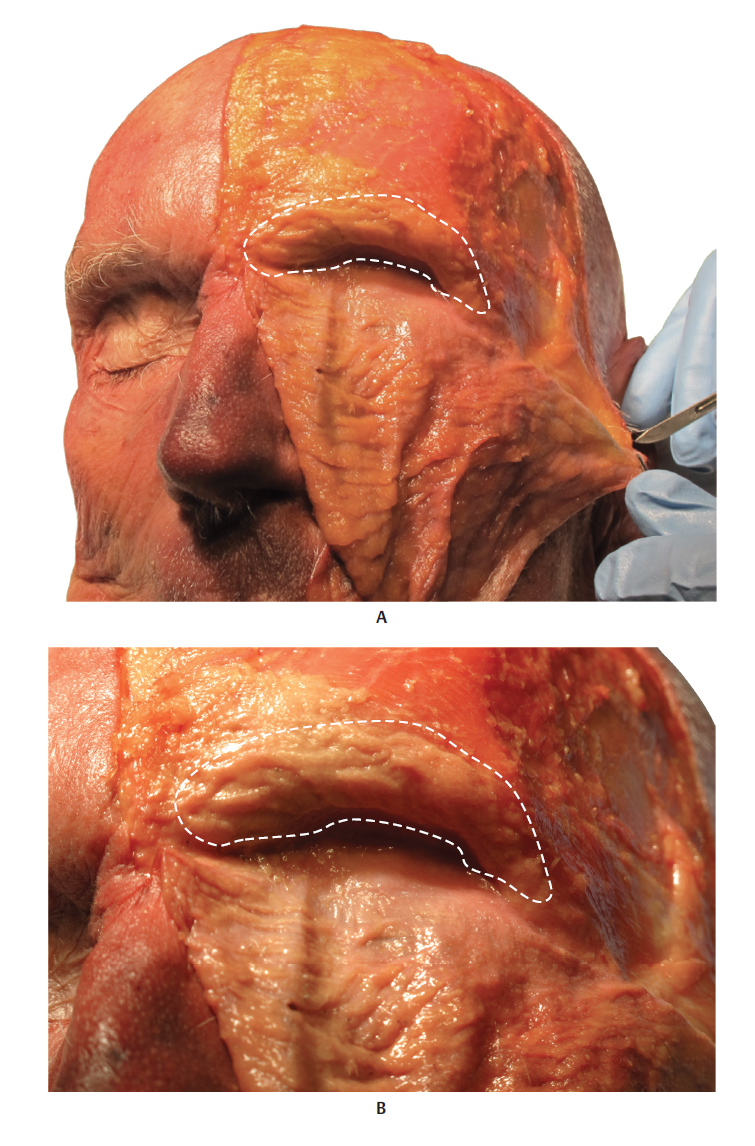
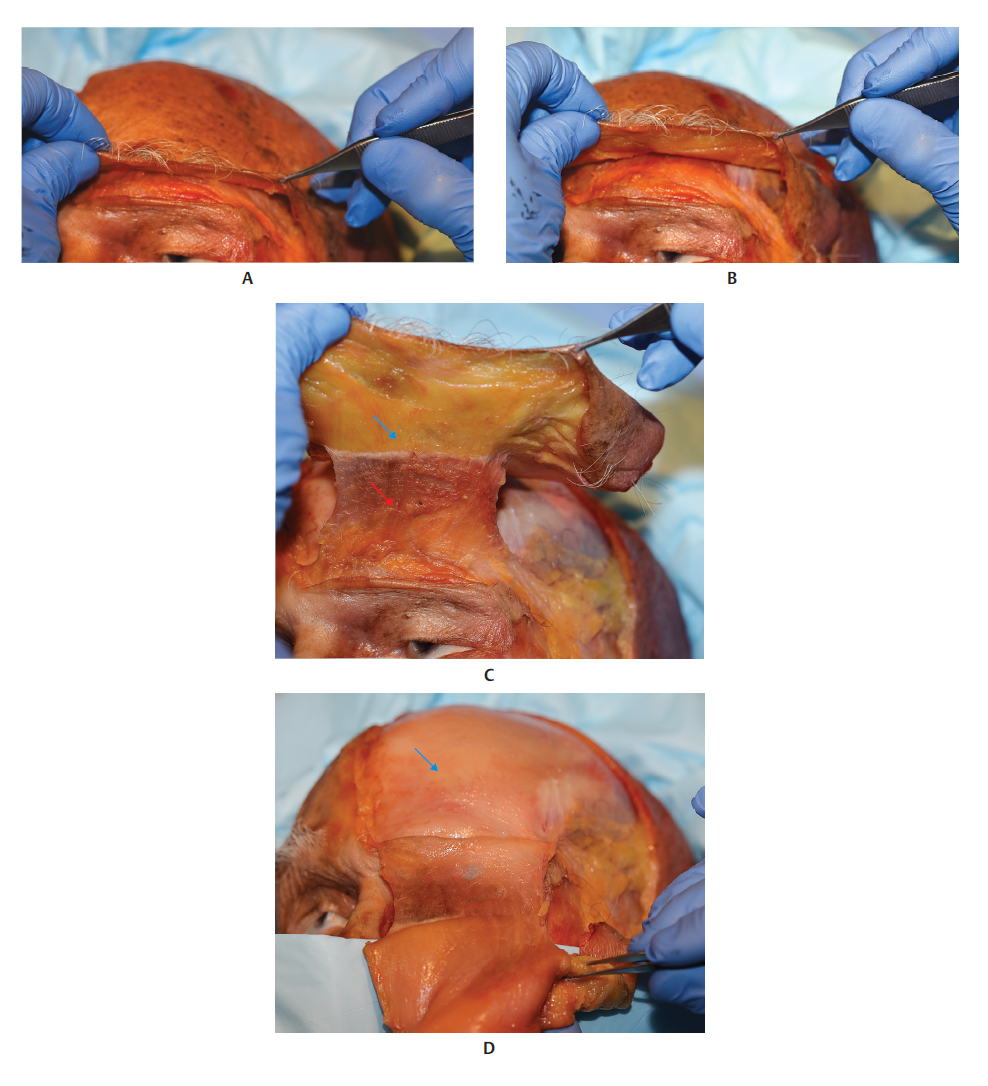
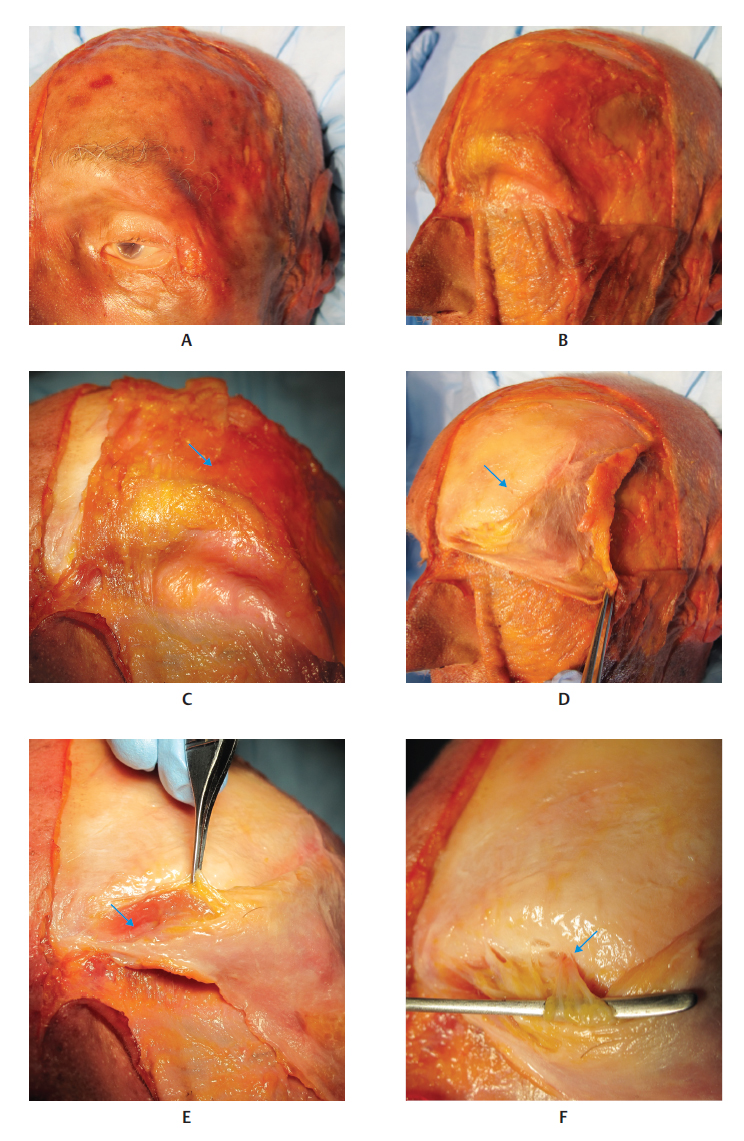
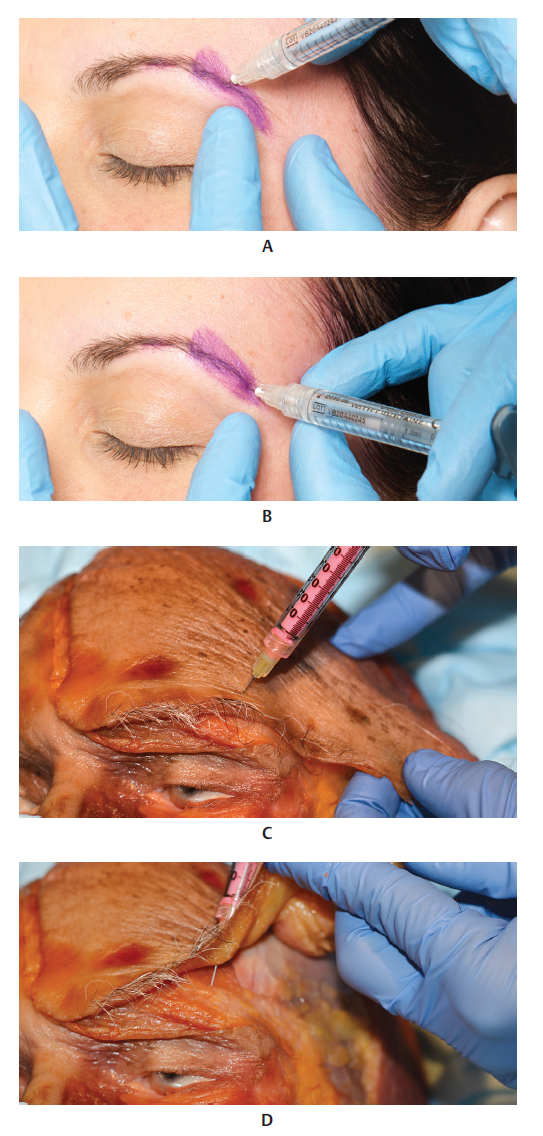
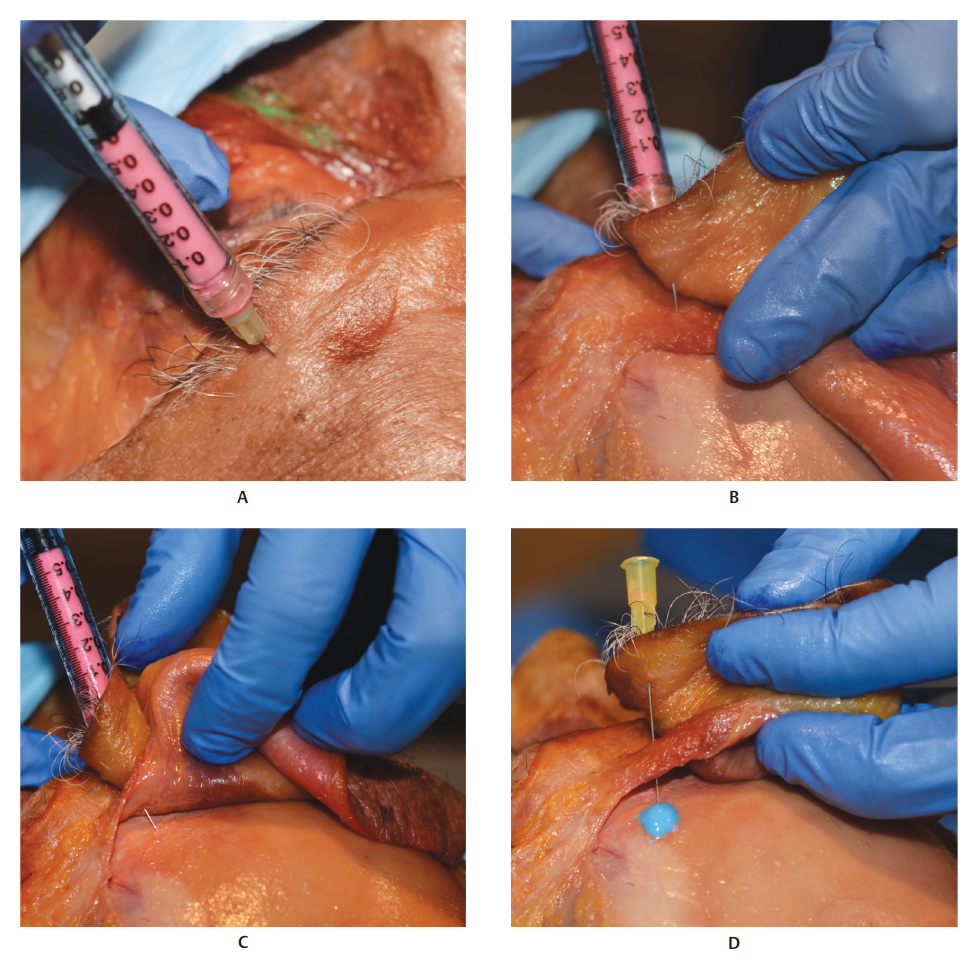
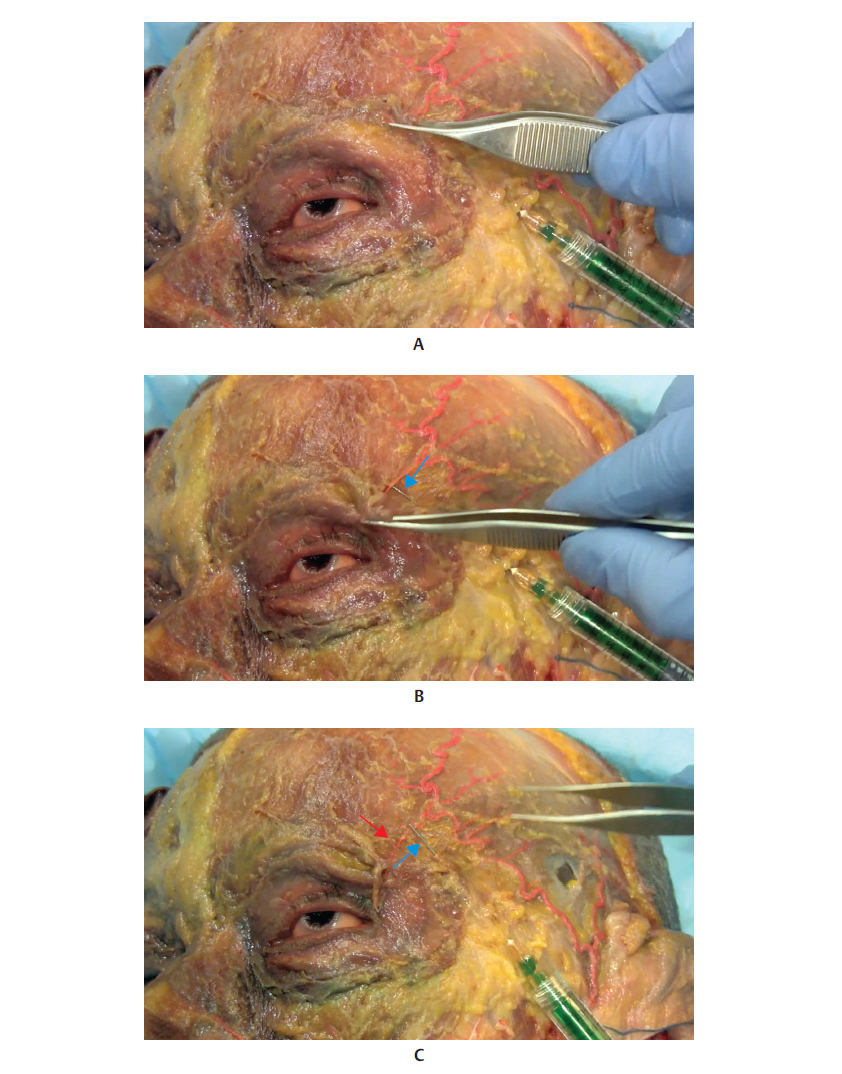
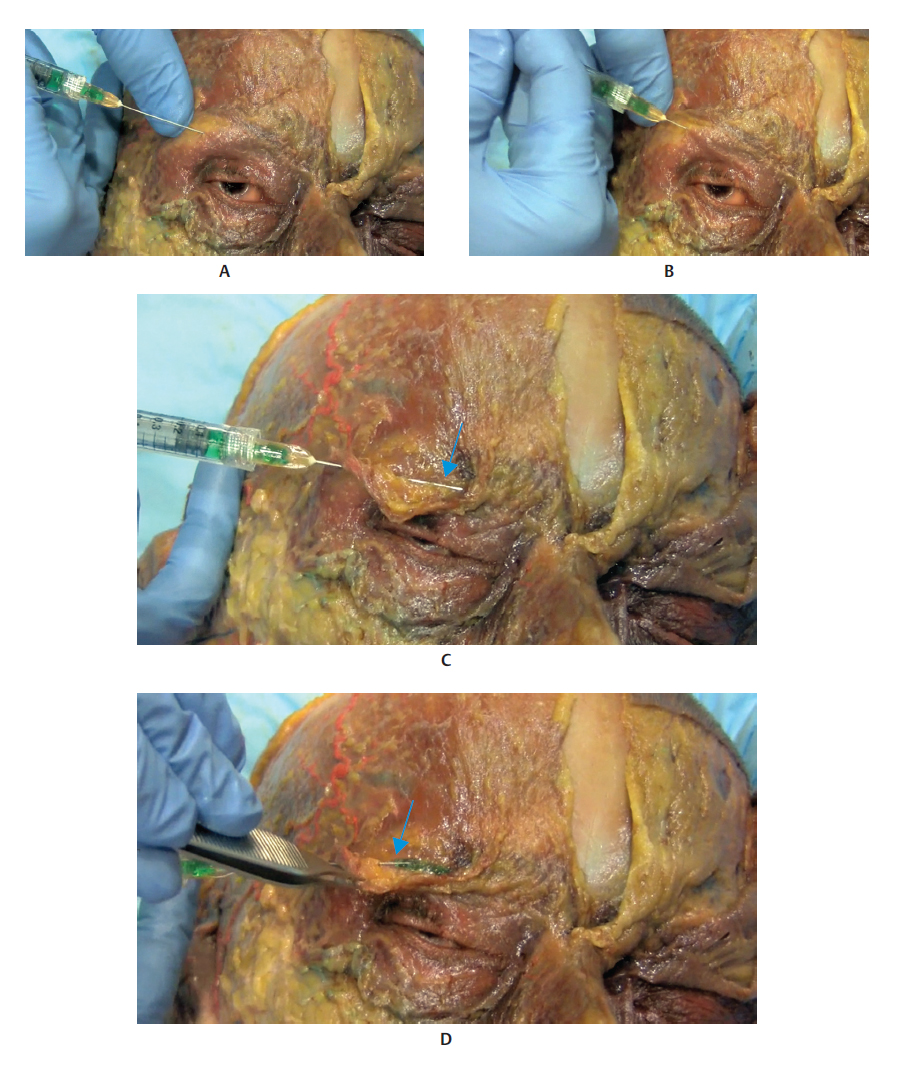
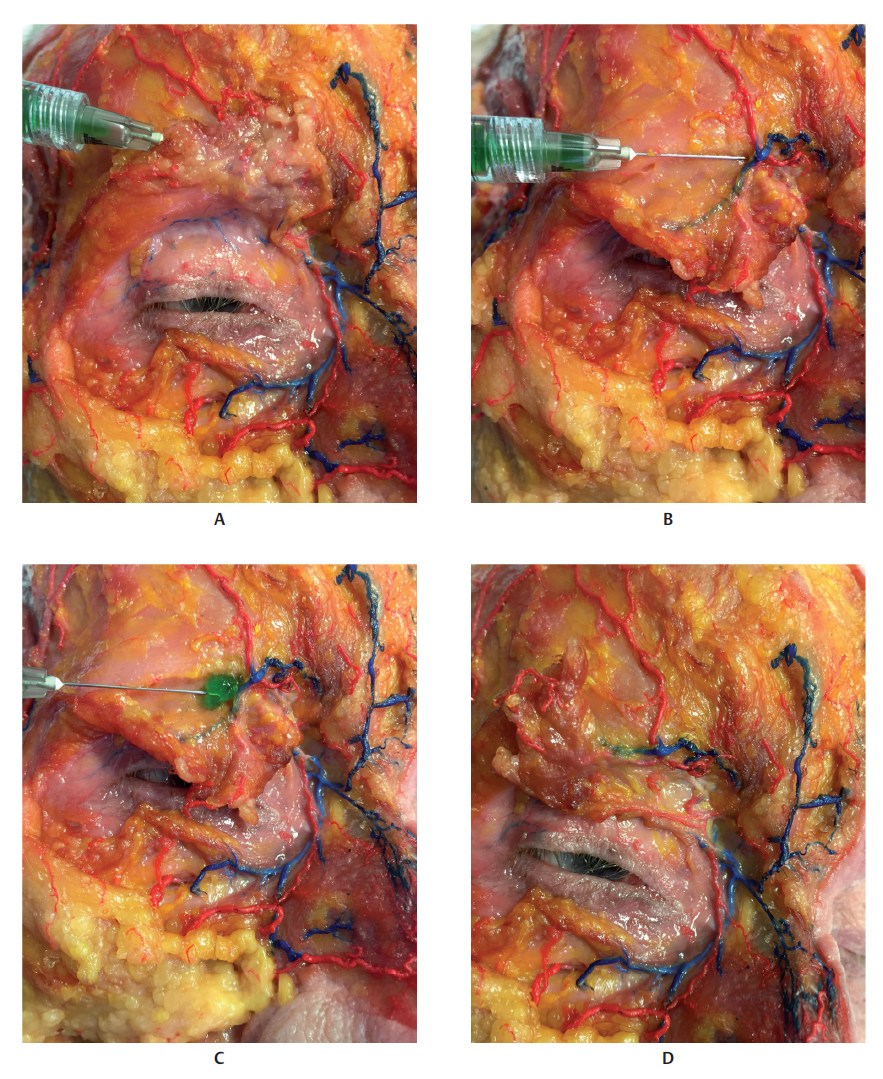
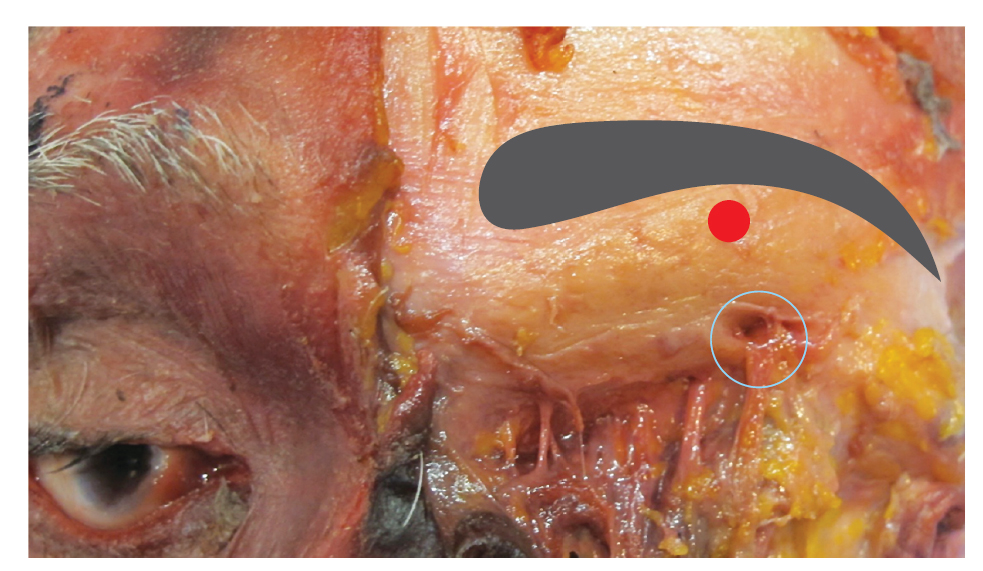
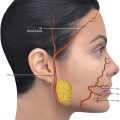
The eyebrow region presents four layers, from the outermost to innermost regions: skin containing sebaceous glands, apocrine glands, and hair follicles; subcutaneous tissue that connects the skin to the aponeurosis of the overlying muscles; superficial layer of the frontal and orbicularis oculi muscles (OMs), and the deep layer, the corrugator supercilii; and the periosteum. 3 Retroorbicularis oculi fat (ROOF) is the deep fat pad located below the orbicular muscle, originating medially at the level of the supraorbital nerve and extending laterally to the superior orbital rim (Fig. 7.2).
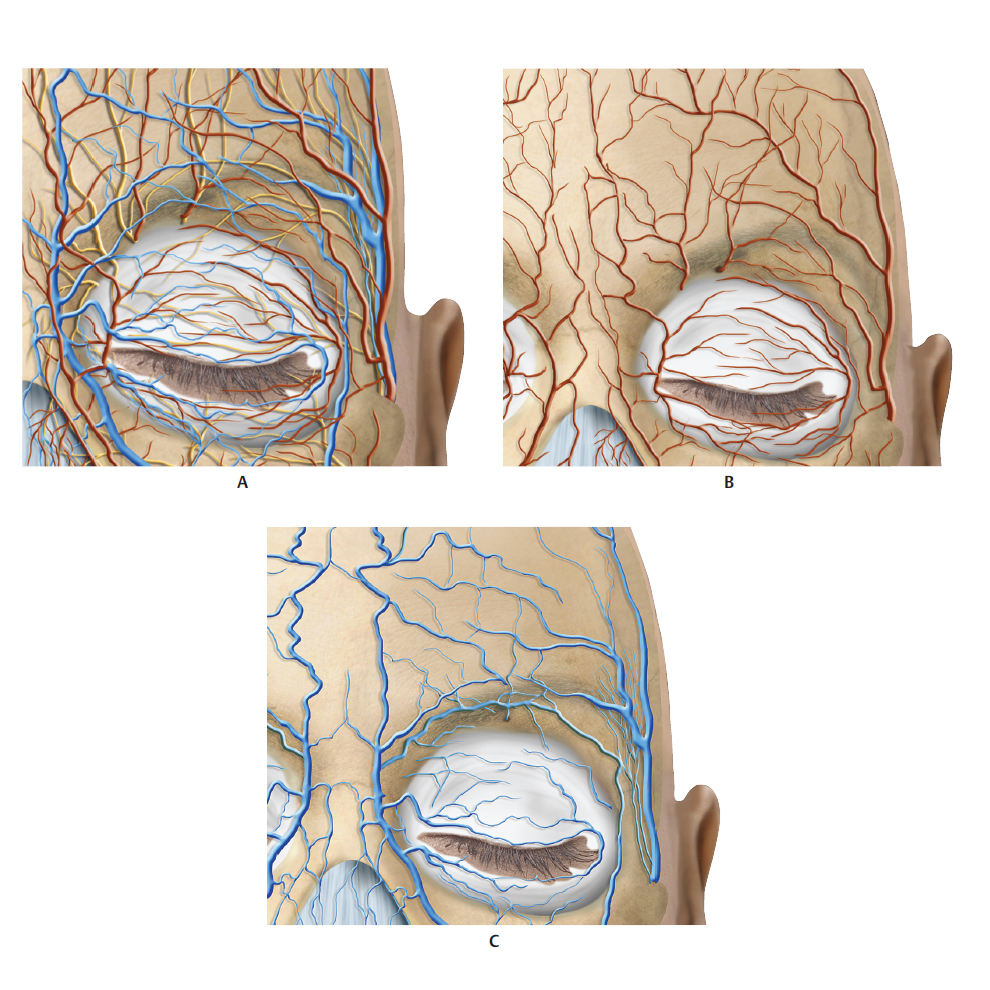
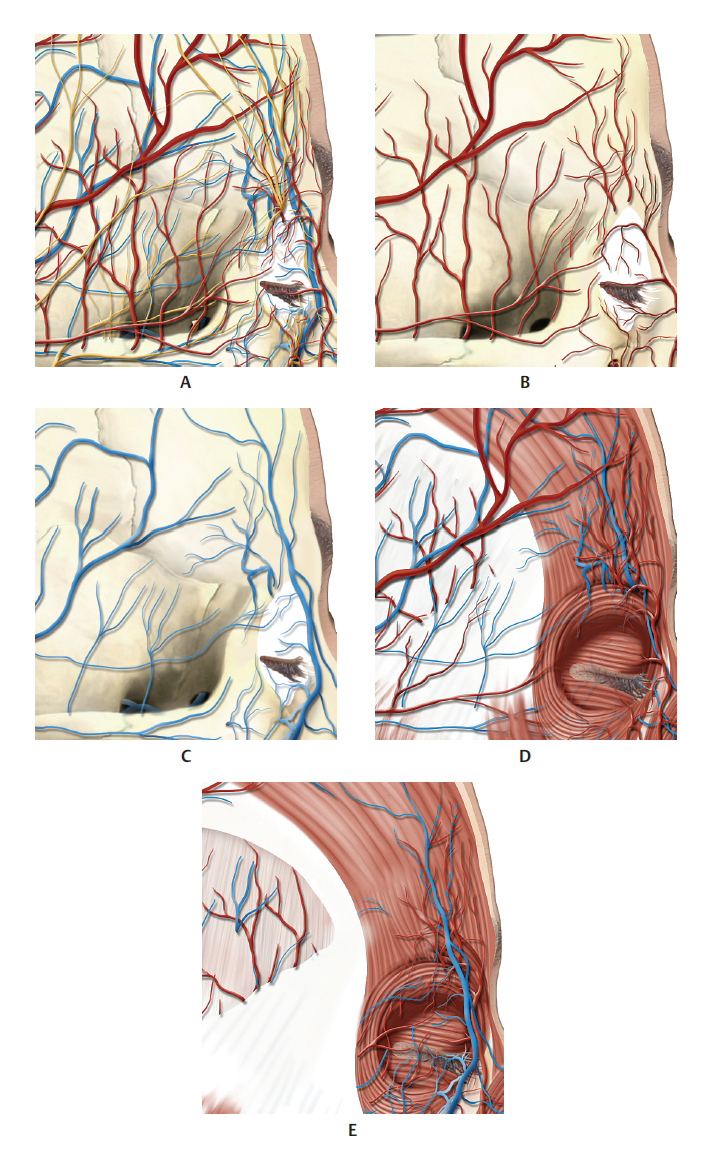
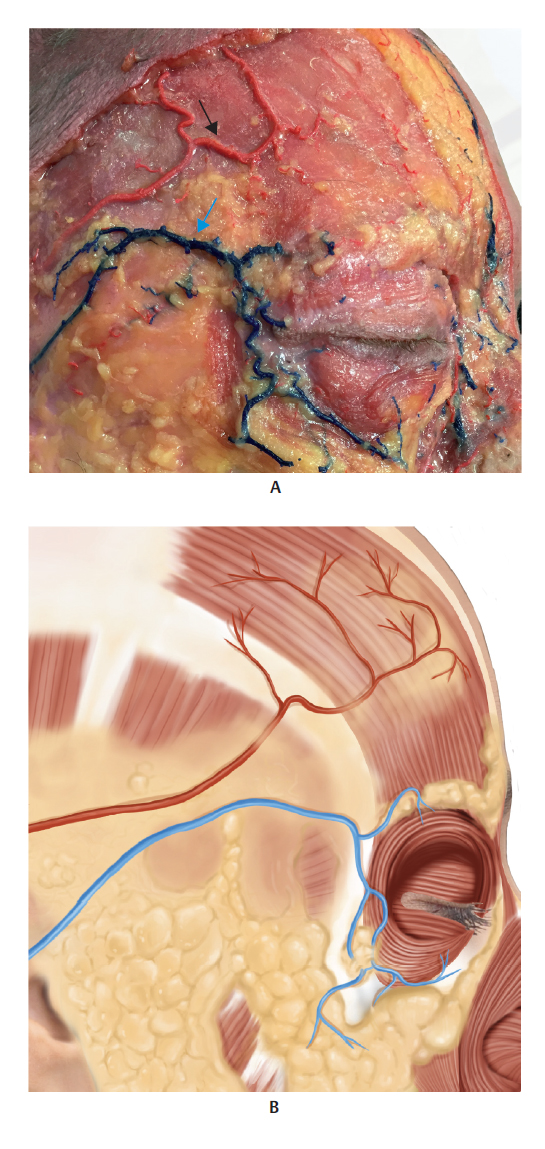
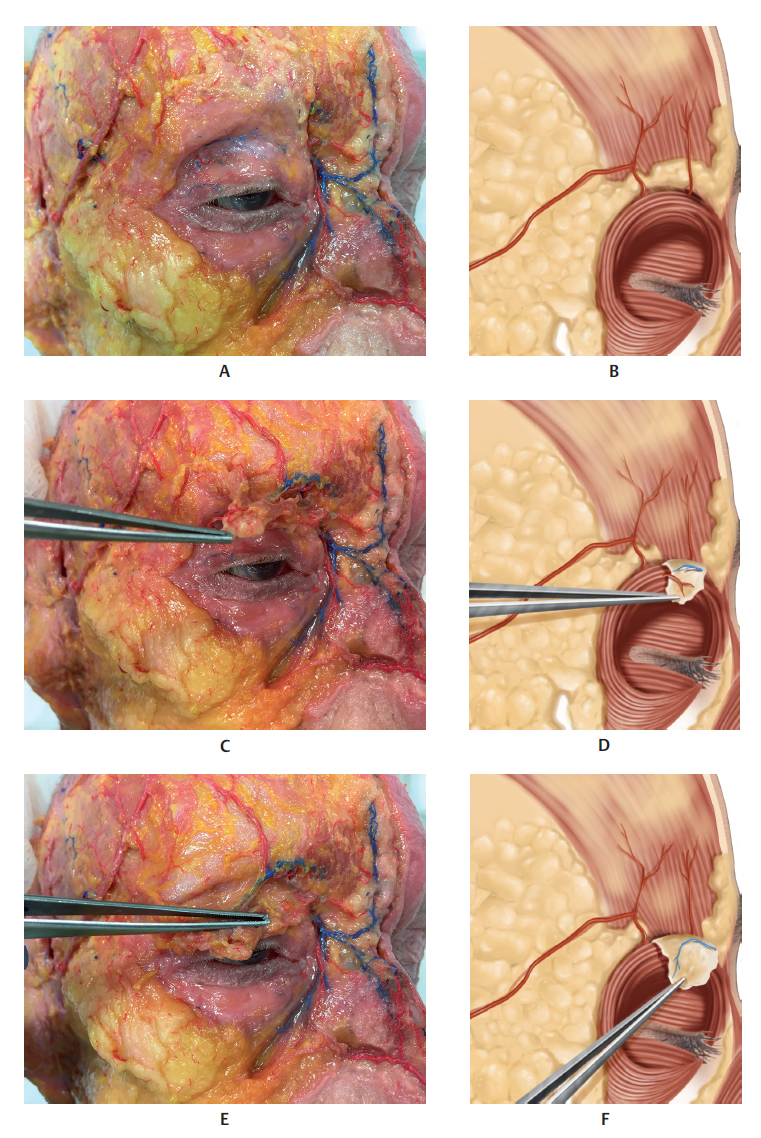
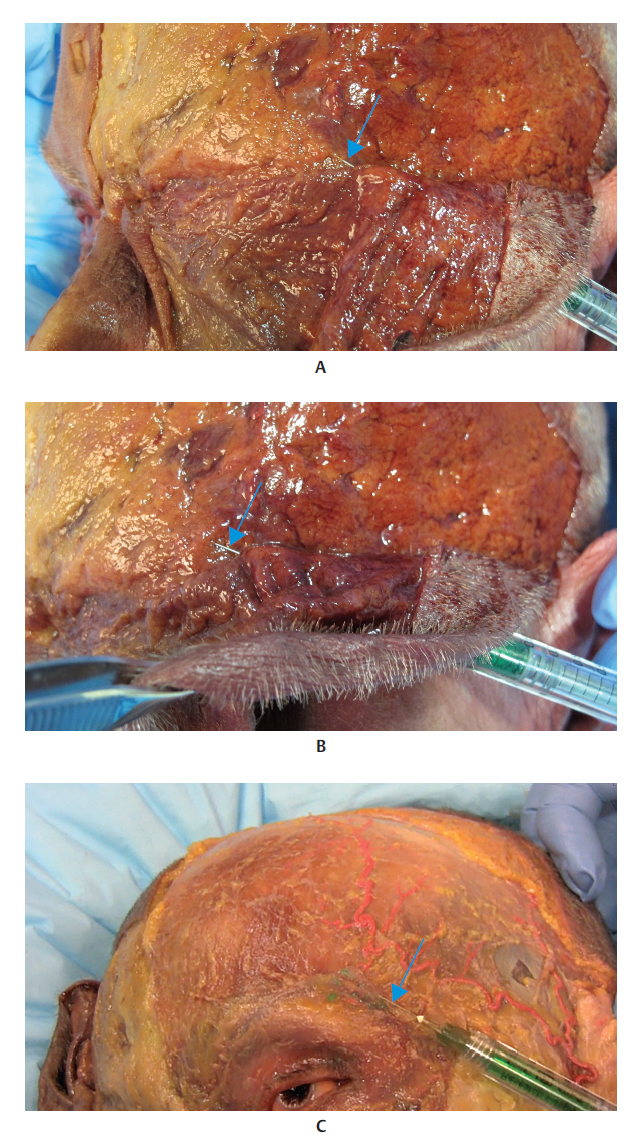
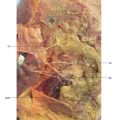
The supraorbital and supratrochlear notches (or foramens in some cases) are located approximately 2.7 and 1.7 cm, respectively, from the midline of the glabella, where the respective vessels and nerves emerge. Caution must be exercised when applying filler injections to this region, as an accidental intravascular injection into one of the distal branches of the ophthalmic artery can lead to a rare but very severe complication consisting of embolization of the central retinal artery, leading to amaurosis. Therefore, in-depth knowledge of the irrigation of the orbital region and its ramifications is important (Fig. 7.3–7.13).
Techniques
References
1 Carruthers J, Carruthers A. Social significance of the eyebrows and periorbital complex. J Drugs Dermatol 2014; 13(1, Suppl):s7–s11 2 Lam VB, Czyz CN, Wulc AE. The brow-eyelid continuum: an anatomic perspective. Clin Plast Surg 2013;40(1):1–19 3 Andre P, Azib N, Berros P, et al. Anatomy and volumizing injections. Paris: E2e Medical Publishing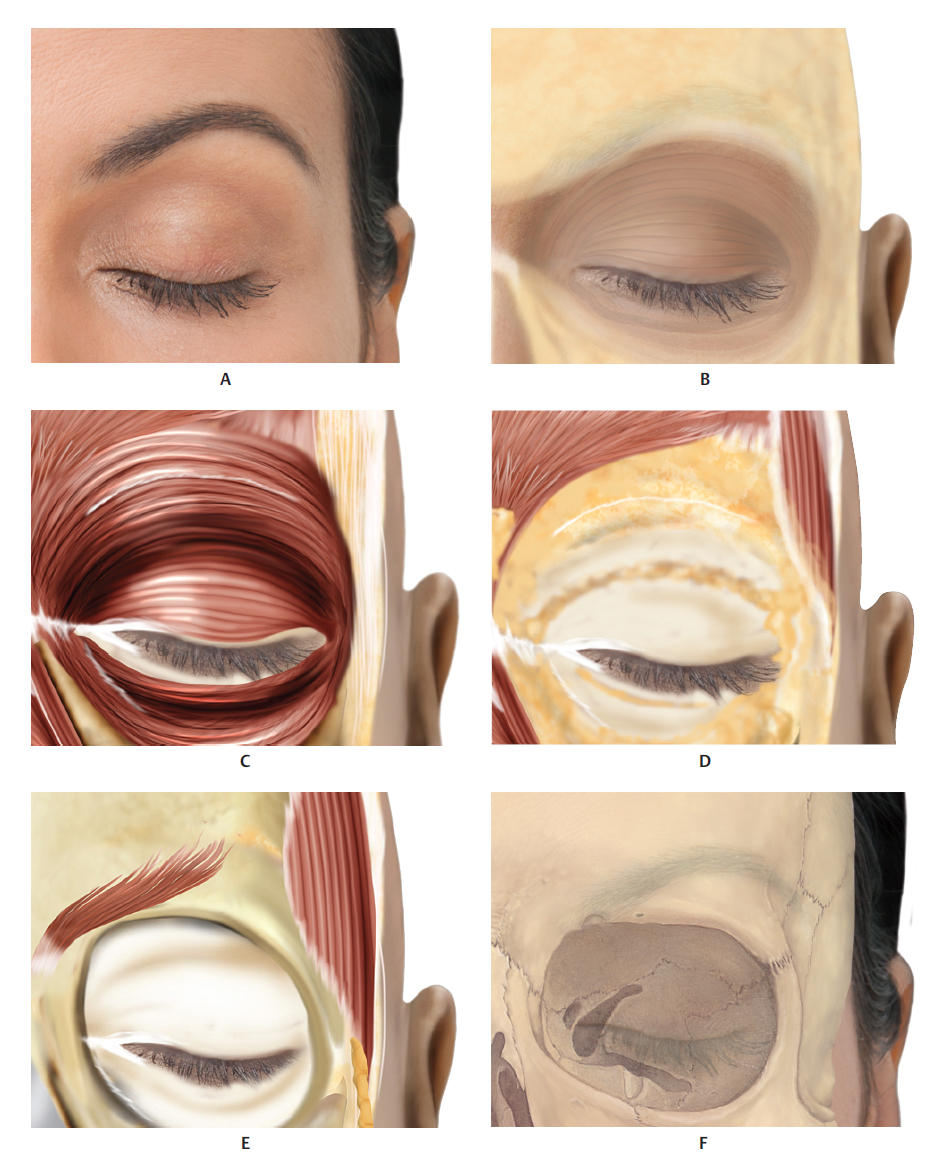





Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


